13 Jun 2016
Veronica Roberts looks at some of the possible causes of weight loss in horses, using gastrointestinal disease as the main focus, and suggests ways of testing for its origin.
Veronica Roberts
Job Title
Figure 4. Laparoscopic-assisted flank laparotomy to biopsy small intestine. Image: Dylan Gorvy and Laura Hirvinen/Strömsholm Equine Referral Hospital.
Significant unplanned weight loss can be a consequence of underlying serious disease. A multitude of causes of weight loss, plus numerous tests, can make investigation seem daunting.
This article gives an overview and guidance of how to start examining these cases, focusing on a detailed investigation of ones where underlying gastrointestinal (GI) disease is suspected.
A practice health care scheme can bring a multitude of benefits. Clearly, being enrolled on a health scheme is unlikely to prevent serious disease, but could help detect weight loss or other signs of the underlying disease early on.
Weight should be taken, and recorded, on each examination. In doing this, the owner can be encouraged to purchase a weight tape and monitor the horse’s weight on a more frequent basis. While weight tapes are not perfectly accurate for actual weight, they will detect fluctuations.
Training your clients to body condition score is also useful. It is possible to have a record of normal haematology and biochemistry values for that individual, making testing in the future more sensitive.
To make a systematic and thorough approach to investigation of a weight loss case, it is first worth structuring your thoughts around possible mechanisms for weight loss.
You can consider the following two schemes; to identify a mechanism of weight loss and, once identified, to seek to identify a cause.
Mechanisms include:
Causes include:
A thorough history and clinical examination may offer an indication of the path to follow with investigations. For example, if the horse also has diarrhoea then further examinations would be targeted towards diseases of the intestinal tract and, if quidding, towards dental/temporomandibular joint disease.
Usually at this stage, most practitioners would accompany history and clinical examination with initial laboratory tests to help determine the direction investigations should take.
Useful information without vast expense can be gained from a thorough haematology, so an initial screen would include total erythrocyte count and differential leukocyte count.
Value exists in the added information available from a blood smear rather than just relying on an in-house machine result. Common anomalies and possible interpretations are anaemia, neutrophilia, neutropenia and lymphopenia/lymphocytosis.
A sensible initial biochemistry would include total plasma solids (albumin plus globulin), albumin, globulin, fibrinogen, liver damage and renal function.
A faecal egg count should be interpreted in conjunction with knowledge of the horse’s parasite management history and the limitations of faecal egg counts as a true measure of the burden of all parasite types. Measurement of faecal occult blood is yet to be proven as a truly specific and sensitive test.
Underlying GI disease is a common cause of weight loss. Pathology of the large intestine may give concurrent signs of diarrhoea, but it should be noted these cases might have concurrent pathology of the small intestine. Some cases will also present with usually chronic or recurrent colic and often hypoalbuminaemia.
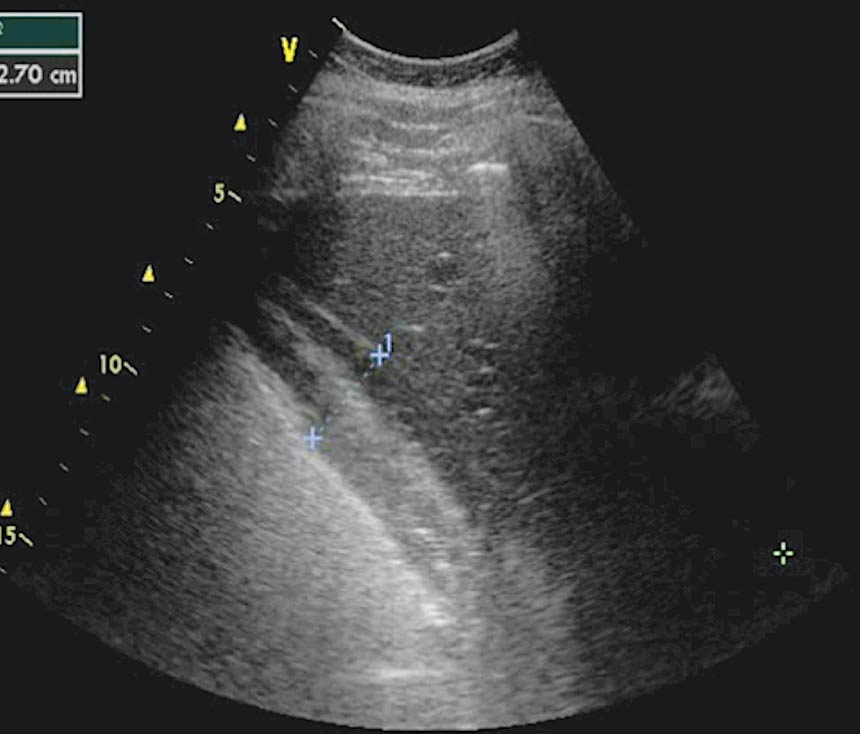
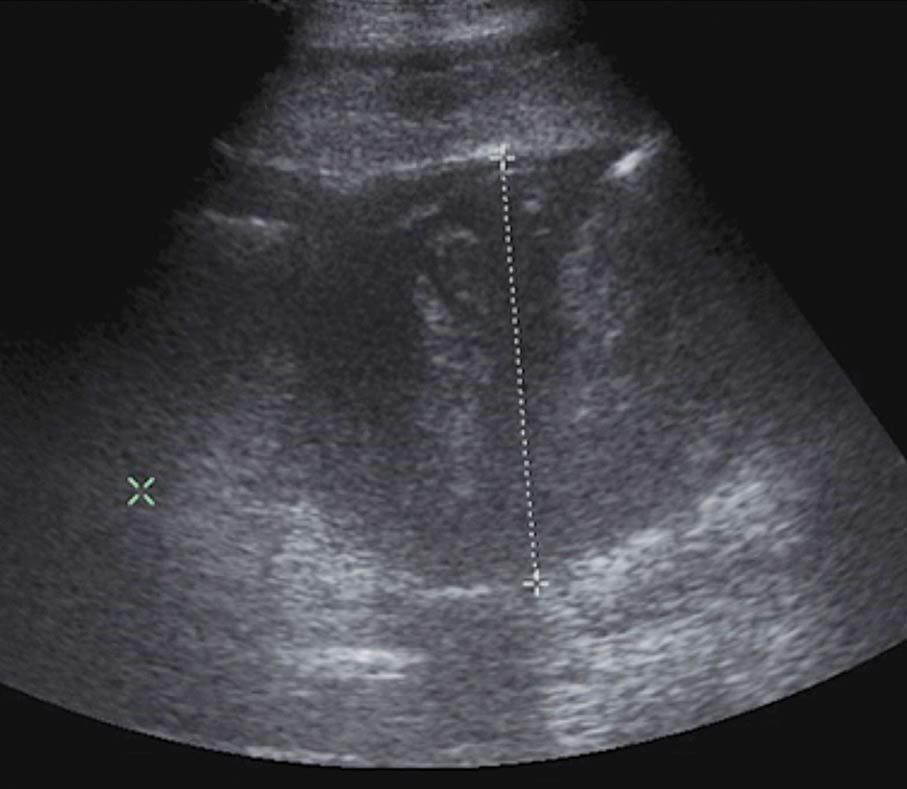
Sensible next steps would include ultrasound, abdominal paracentesis, glucose absorption test and biopsy.

Many possible causes of weight loss exist and various tests can be taken, so aim for a targeted approach, using tests in a step-wise fashion, rather than a scatter-gun approach.