24 Jul 2017
Lara Gosling, Jonathon Dixon and David Rendle – in the first of a two-part article – review sampling of the lower airway tract.
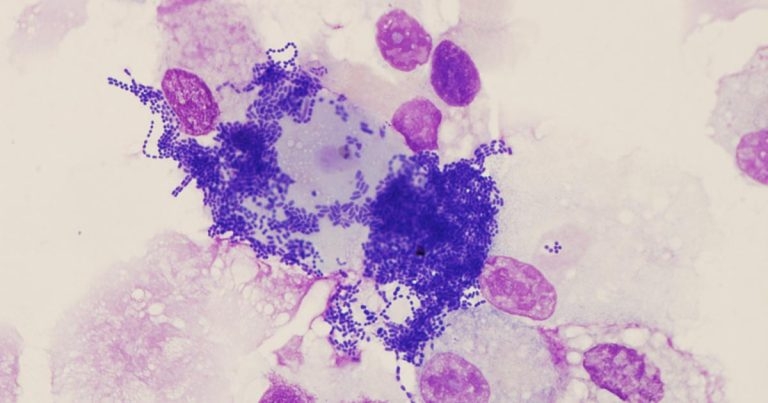
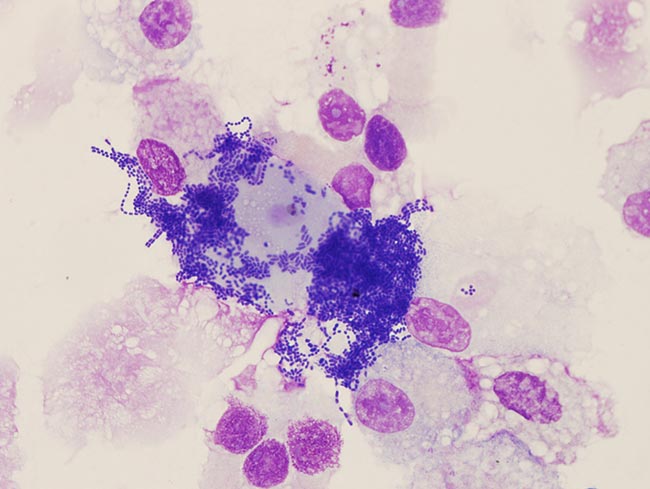
Figure 6. Extensive contamination in a sample of tracheal aspirate fluid.
Lower respiratory tract disease is common in equine practice, with 45% of owners reporting in one study their horse had previously suffered from a cough (Hotchkiss et al, 2007). In a population of leisure horses, 83% had cytological evidence of lower airway inflammation in bronchoalveolar lavage fluid (BALF; Wasko et al, 2011).
In the UK, the National Equine Health Survey reported a respiratory disease prevalence of 5% (Slater, 2014). The spectrum of inflammatory lower airway disease, now reclassified as equine asthma (Couëtil et al, 2016), ranges from mild equine asthma (formerly inflammatory airway disease) – in which clinical signs are not apparent at rest – to marked equine asthma (formerly recurrent airway obstruction; heaves) where there may be marked respiratory distress (Figure 1).

Lower airway washes should be considered for all cases of lower respiratory disease and may also be indicated in cases presenting with pyrexia of unknown origin or poor performance. A tracheal wash or aspirate samples the larger airways, while a bronchoalveolar lavage samples the smaller, more distal airways. Performing both techniques in one sampling period is strongly recommended, as each provides information the other cannot. Identification of neutrophilia in BALF is the gold standard test for diagnosis of lower airway inflammation (Couëtil et al, 2016; Cian et al, 2015).
Poor correlation exists between BALF cytology and both tracheal aspirate fluid (TAF) cytology and tracheal mucus grading (Gerber et al, 2003; Fraipont et al, 2011), so visualisation and sampling of the trachea alone is not sufficient to fully assess lower airway inflammation.
Respiratory tract sampling may not be appropriate in cases with acute respiratory distress and, in such cases, should be postponed until respiratory function improves.
If respiratory disease has not been localised to the lower respiratory tract, thorough assessment of the nasal passages, nasopharynx, guttural pouches, trachea and carina should be performed. Laryngeal function (unsedated), discharge from either the sinus drainage angle or guttural pouches, and pharyngeal lymphoid hyperplasia should all be noted. After a tracheal aspirate has been collected, the endoscope can be advanced to the distal trachea so the carina and mainstem bronchi can be assessed.
The quantity of mucus in the trachea is assessed endoscopically (Figure 2) and a subjective grade (Gerber et al, 2004) applied as follows:
Due to the efficiency of the mucociliary escalator in normal horses, little or no mucus should be present in a healthy respiratory tract.
Tracheal aspirates may be collected via transendoscopic and transtracheal methods. A transtracheal aspirate is indicated where a sterile sample needs to be obtained – for example, cases of pleuropneumonia. However, it is invasive and carries a risk of infection at the incision site, so is less commonly performed – especially when good transendoscopic technique minimises the risk of sample contamination (Christley et al, 1999).
A transendoscopic tracheal aspirate allows visualisation of the airways and grading of the mucus present (Allen and Franklin, 2007). It is essential the tip of the endoscope remains proximal to the fluid pool prior to sampling to prevent contamination with oropharyngeal bacteria.
To perform a tracheal aspirate:
Once the sample has been collected, the catheter can be withdrawn, and the carina and mainstem bronchi can be examined. If a BAL is also to be performed, lidocaine can be instilled around the tracheal bifurcation and larynx before the scope is withdrawn.
Bronchoalveolar lavage (BAL) provides more reliable information on peripheral airway disease and correlates well to clinical findings in inflammatory airway disease (Hoffman, 2008). Variability in TAF cytology results can be significant, with little correlation between TAF cytology and pulmonary histopathology in cases with lower airway disease (Larson and Busch, 1985; Winder et al, 1989), so BAL should always be performed in cases with suspected lower airway inflammation (unless the animal is in acute respiratory distress). Bacteriological assessment is rarely performed on BAL samples due to inevitable contamination as the tube passes through the oropharynx (Hodgson and Hodgson, 2007).
Performing a BAL requires the horse to be sedated, ideally with butorphanol included in the sedation protocol for its antitussive effects (Cavanagh et al, 1976). Administration of lidocaine either via an endoscopic catheter or through the nasobronchial tube into the lower airways may reduce coughing. A BAL can be performed using a cuffed nasobronchial tube or via an endoscope. Coughing should be expected as the endoscope/tube reaches the carina and the owner should be warned of this prior to commencing the procedure. Endoscopic BAL may be preferred if a specific region is to be sampled. However, in equine asthma, pathology is typically distributed equally throughout the pulmonary parenchyma and, although regional aspiration may yield samples with slightly differing cytological profiles, this is unlikely to alter the clinical interpretation (Mazan, 2015; Kutasi et al, 2011).
After a BAL, the horse should be rested for 24 hours.

At least half of the instilled volume should be collected to ensure the resultant sample is representative of the distal airways, and not just of the area local to the tube tip. The sample should be foamy, indicating the presence of a surfactant and, hence, that adequate lavage of the alveoli has been performed (Hoffman, 2008; Figure 4).

Samples for cytology should be chilled and analysed as soon as practical to minimise cell deterioration and bacterial growth. It is good practice to prepare, fix and send a smear concurrently to give the laboratory a reference for bacterial growth and sample degradation. Fluid samples should be chilled in transit (Pickles et al, 2002). Samples for bacteriology should not be placed in a preservative or fixative, but kept plain and transported chilled to the laboratory.
Gross examination of the sample provides further subjective information of the quantity of mucus present and, hence, an indication of airway inflammation (Figure 5). Normal samples will be clear or mildly grey and turbid. Increased turbidity or the presence of flocculent material indicates increased mucus and cellular material in the sample. Frank blood may be seen consistent with recent haemorrhage – typically as a result of exercise-induced pulmonary haemorrhage (EIPH) – or a brown sample may indicate the presence of less recent haemosiderin and haemorrhage. Plant material indicates contamination and a need for caution when interpreting the results of bacterial culture.

White cell differential counts are the most important factor to consider when interpreting lower airway cytology. Absolute values are affected by dilution, which cannot be quantified and are, therefore, unhelpful. Epithelial cells should not be considered as part of the differential count.
Reference values for relative proportions of leukocytes in tracheal aspirate and bronchoalveolar lavage fluid are as follows:
| Cell type | TA (%) | BAL (%) |
| Macrophages | 40-80 | 40-70 |
| Lymphocytes | Less than 20 | 30-60 |
| Neutrophils | Less than 20 | Less than or equal to 5 |
| Eosinophils | Less than 1 | Less than 1 |
| Mast cells | Less than 1 | Less than 1 |
| (Hoffman, 2008; Richard et al, 2010; Couëtil et al, 2016). | ||

An increased proportion of neutrophils is the most consistent indicator of lower respiratory tract inflammation.
Bacteriology should always be interpreted carefully, with consideration for contamination from collection – for example, from the end of the endoscope entering the fluid pool within the trachea or coughing during the procedure. Contamination is indicated by the presence of foreign material or oropharyngeal squamous epithelial cells (Figure 6). The presence of bacteria is considered significant if:
Bacterial species is important. Many species that are isolated commonly are known contaminants and their presence is not relevant clinically. Antimicrobial susceptibility should only be performed and acted on if the bacterial isolate is likely to be pathogenic. Bacteria commonly isolated from tracheal aspirates and their likely pathogenicity are as follows:
Likely pathogens
Likely contaminants
(Source: Hodgson and Hodgson, 2007).