4 Nov 2019
Sue Dyson describes work to assess if facial expression or behaviour can help determine presence of this pain.
Sue Dyson
Job Title
Many horses appear sound in hand, but have underlying pain-related musculoskeletal problems when ridden. However, horses show a variety of gait modifications in an attempt to reduce pain and minimise lameness, including reducing range of motion of the thoracolumbosacral region1, taking shorter steps, alteration of limb flight and increasing body lean2.
It is apparent owners, riders and trainers have a poor ability to recognise signs of pain that manifest when horses are ridden. In a study of 506 sports horses in normal work and presumed to be sound, 47% were overtly lame, or had other pain-related gait abnormalities (for example, stiff, stilted canter)3. As a result, problems are often labelled as training-related, rider-related or behavioural – or as “that is just how the horse has always gone”. Consequently, pain-related problems often get insidiously, but progressively, worse.
Many veterinarians have had little training in pain recognition and limited education in identification of low-grade lameness, especially in ridden horses. Therefore, many struggle to recognise musculoskeletal pain as a cause of poor performance. Owners are frustrated when they think their horse has an underlying pain-related problem, but are informed by their veterinarian no detectable lameness is notable and the problem must be “behavioural”.
They become even more frustrated if the horse is subjected to whole-body scintigraphy, providing either negative or false-positive results. It has been demonstrated screening in such circumstances is highly unlikely to yield useful results4.
It would, therefore, be useful to have additional tools for owners, trainers, veterinarians and other paraprofessionals to help them recognise signs of musculoskeletal pain. We have recognised certain behavioural signs that appear to reflect pain in horses by comparison of clinically sound horses and those with musculoskeletal pain – and horses with musculoskeletal pain before and after diagnostic analgesia has improved lameness; for example, unwillingness to go, bolting or head tossing.
We postulated these relatively easily observed signs might be used to develop a ridden behaviour ethogram that could improve the ability of minimally trained observers to differentiate horses with musculoskeletal pain from those with other behavioural, training or rider problems4. However, this requires evidence-based validation and the aim of this paper is to describe some of the steps that have been taken towards this.
We have completed several parts of a multiphase study. In part one, we assessed the ability of people from a range of professional backgrounds to assess facial expressions of ridden horses based on still photographs of the head5. The objectives were to develop and test an ethogram to describe facial expressions in ridden horses, and to determine whether individuals could interpret and correctly apply the ethogram, with consistency among assessors.
An ethogram was developed in conjunction with Jeannine Berger, a diplomate of the American College for Veterinary Behaviorists and the American College of Veterinary Welfare, by reference to previous publications, and photographs of 150 lame and non-lame ridden horses. A training manual was also created. Thirteen assessors (veterinarians of variable experience, n=4; equine technicians, n=3; equine studies graduates, n=2; amateur horse owners, n=2; an equine veterinary nurse, n=1; and a British Horse Society instructor, n=1) underwent a training session and, with reference to the training manual, evaluated still, lateral photographs of 27 training heads.
Features were graded as yes, no or “cannot see” (when it was not possible to determine the presence or absence of a feature). The ethogram was adapted and, after further training, the assessors blindly evaluated 30 test heads from non-lame and lame horses. Intra-class correlation (ICC) and free-marginal kappa tests were used to assess consensus among assessors.
For the training heads, single ICC matrix among observers resulted in an overall ICC of 0.50 (95% confidence intervals, 0.40 to 0.62). Four assessors consistently scored differently from the others, with ranges of ICC of 0.20 to 0.50 (mean 0.41). No difference was seen in assessors’ scoring related to their professional backgrounds.
For the test heads, mean rater agreement among assessors was 87%. Two assessors still scored consistently differently (0.28 to 0.50 ICC agreement; mean 0.40) from the remaining 11 assessors (0.44 to 0.69 ICC agreement; mean 0.56). The mean percentage of overall agreement was 80% and the mean free-marginal kappa value was 0.72, standard deviation (SD) ± 0.22.
The large SD was the result of inconsistency in assessments of the eyes and muzzle. It was concluded the developed ethogram could reliably be used to describe facial expressions of ridden horses by people from different professional backgrounds. Training enhanced accuracy of application of the ethogram.
In part two, the objective was to determine if, based on assessment of still photographs of the heads of normal (non-lame) horses and lame horses (including some before and after diagnostic analgesia abolished lameness) undergoing ridden exercise, differentiation could be made between those horses experiencing pain and those that were non-lame6.
It was hypothesised lame horses would have higher pain scores than non-lame horses; and that the pain score of lame horses would be reduced after abolition of pain by diagnostic analgesia. The previously developed facial expression for ridden horses (FEReq) ethogram was applied blindly by a trained analyst to photographs of the head and neck of lame (n=76) and non-lame (n=25) horses acquired during ridden schooling-type work at both trot and canter. These included images of seven lame horses acquired before and after diagnostic analgesia had abolished lameness. Each horse had to have a minimum of 10 images reflecting the spectrum of facial expressions exhibited during a work period. A pain score (0 to 3; 0=normal, 1 to 3=abnormal) was applied to each feature in the ethogram, based on published descriptions of pain in horses.
Pain scores were higher for lame horses than non-lame horses (p<0.001). Total pain score (p<0.05), total head position score (p<0.01) and total ear score (p<0.01) were reduced in lame horses after abolition of lameness. Severely “above the bit”, tilting the head, asymmetrical position of the bit, ear position (both ears backwards, one ear backwards and one to the side, one ear backwards and one ear forwards) and eye features (exposure of the sclera, the eye partially or completely closed, muscle tension caudal to the eye, an intense stare) were the best indicators of pain.
Application of the FEReq ethogram and pain score could reliably differentiate between lame and non-lame horses. It was concluded that assessment of facial expression could potentially improve recognition of pain-related gait abnormalities in ridden horses6,7.
For 25 lame horses, images were available of the horse standing still with a rider on; the scores were significantly lower than for both the non-lame horses and the lame horses when ridden, indicating the changes in facial expression were not the mere effect of rider weight, but were the response to ridden exercise. It has been suggested mouth opening may be the result of the presence of a bit. However, the frequency of mouth opening when being lunged wearing a bridle, with the lunge rein attached via couplings to the bit, was substantially less than when the same horses were ridden, indicating mouth opening was a consequence of being ridden.
In part three, we aimed to develop an ethogram for whole-horse behaviour of ridden horses to assess its repeatability, and to determine whether the ethogram could be used to differentiate between non-lame and lame horses8. It was hypothesised that:
The ethogram was developed with 117 behavioural markers (including FEReq markers), each with strict definitions, and horses were graded twice in random order by a trained analyst using video footage. Overall, good correlation was noted between two assessments of nine horses (p<0.001; R2=0.91). Unreliable behavioural markers were omitted, reducing the ethogram to 70 markers. The modified ethogram was applied to video recordings of non-lame horses (n=13) and lame horses (n=24; ethogram evaluation).
Strong correlation was noted between 20 behavioural markers and the presence of lameness. The ethogram was subsequently simplified to 24 behavioural markers, by the amalgamation of similar behaviours that scored similarly and by omission of markers that showed unreliable results in relation to lameness.
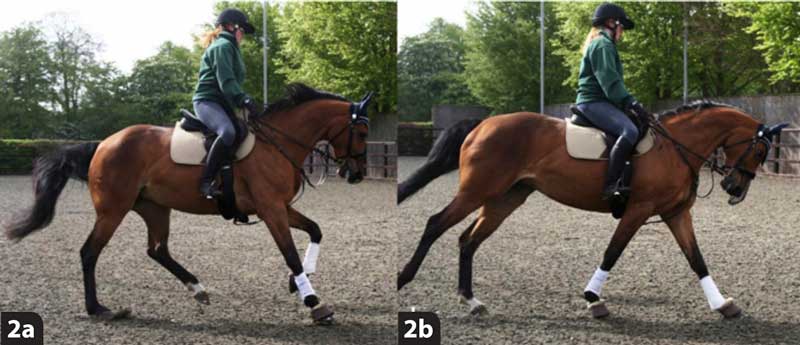
The final ethogram comprising 24 behaviours was applied to 13 non-lame horses and 24 lame horses by a trained analyst. The maximum individual occurrence score for lame horses was 14 (out of 24 possible markers), with a median score of 9 and a mean score of 9 (SD±2) compared with a maximum score of 6 for non-lame horses, with a median and a mean score of 2 (SD±1.4). For lame horses, the following behaviours occurred significantly more frequently than in non-lame horses (p<0.05, Chi-square): ear(s) back for ≥5 seconds, mouth opening for ≥10 seconds, tongue out, change in eye posture and expression, going above the bit (front of head >30⁰ in front of vertical for ≥10 seconds), head tossing, tilting the head, unwillingness to go, crookedness, hurrying (≥40 trot steps/15 seconds), changing gait spontaneously, poor quality canter (on three tracks, changing legs spontaneously repeatedly, breaking), resisting and stumbling and toe dragging (Figures 1a and 1b).

To provide further evidence that the behaviours were a reflection of musculoskeletal pain, video recordings of 10 lame horses were reviewed blindly in random order by a trained assessor before and after diagnostic analgesia resolved the baseline lameness and improved any gait abnormalities seen in canter9. The ridden horse ethogram was applied to each horse under each circumstance it was ridden. The same rider rode before and after diagnostic analgesia – a repeated measures design. Occurrence (yes/no) for each of the 24 behaviours was recorded.
The mean and median scores before diagnostic analgesia were 12.1 and 12, respectively (range 6 to 24). After lameness resolution, the mean and median scores reduced to 5.9 and 5 respectively (range 3 to 10). After abolition of lameness, the total sum score of behaviours (P<0.01), sum of facial (P<0.05), sum of body (P<0.05) and sum of gait (P<0.05) scores were all significantly reduced (Figures 2 and 3). Fifteen behavioural markers occurred significantly more often in lame horses (P values of 0.00 to 0.05) and an additional four markers were only seen in lame horses. The marked reduction in behaviour scores following resolution of lameness verified a causal relationship between musculoskeletal pain and the behaviour markers.

It was concluded the presence of 8 or more of the 24 behaviour markers was likely to reflect musculoskeletal pain.
None of the horses in the present studies had evidence of oral pain. Saddle fit was assessed in all horses; if poorly fitting, the owner’s saddle was replaced by a better-fitting saddle before acquisition of the post-analgesia video recordings. A number of features were not assessed, but they are of potential clinical relevance. Tooth grinding, abnormal breathing noises and grunting were not evaluated because they could not be heard reliably from the video recordings.
Disproportionate sweating relative to the level and amount of work and fitness was not recorded, although this has been observed in lame horses, disappearing after abolition of pain using diagnostic analgesia. Features that may be felt by a rider: episodic shooting forwards; absence of rein tension (not taking a contact); symmetrically increasing rein tension (hanging on the reins); asymmetrical rein tension (hanging on one rein more than the other); reduced range of motion of thoracolumbosacral region (“back stiffness”); tension; lack of hindlimb impulsion; and being on the forehand.
Features of gait that are difficult to reliably measure without high-speed video include alterations in canter (for example, temporal and spatial separation of the hindlimbs during the stance phase). Definitive differentiation between pain or discomfort induced by tack and other innate behavioural reasons cannot be made on the basis of this study. When a horse is learning a new movement, it may misunderstand the rider’s cues or find it physically difficult due to the unaccustomed use of specific muscle groups, which may result in delayed onset muscular stiffness, while resistant behaviour may be displayed. However, persistence of such behaviours would not be expected unless an underlying pain-related problem was present.
To acquire an accurate behaviour score, it is important to observe horses from all perspectives (from in front, behind and the side) performing at least trot and canter, and transitions between gaits – both going around an arena periphery and performing 10-metre diameter circles in rising trot. Some horses show more signs consistent with pain in canter compared with trot, or vice versa. However, in some horses, pain may only manifest when more specialised and physically demanding movements (for example, collected trot half-pass and canter flying changes) are performed. So, inclusion of these in the assessment for selected horses is recommended.
We use this ethogram daily; the demonstration of ≥8 behavioural markers in a 5-minute work period is likely to reflect musculoskeletal pain. However, some overlap is seen between lame and non-lame horses, and some lame horses score <8. Persistence of ≥8 behavioural markers after lameness is abolished using diagnostic analgesia is likely to reflect a concurrent problem meriting further investigation, such as a poorly fitting saddle or sacroiliac joint region pain.
Part two looks at the ability of non-trained assessors to apply the ridden horse ethogram to video recordings, investigate the ability of veterinarians to apply the ethogram in real time to lame and non-lame horses, and compare real-time application of the ethogram by a trained analyst with video assessment.