23 Jun 2026
Andy Durham BVSc, BSc, CertEP, DEIM, DipECEIM, MRCVS discusses testing, prevention and management options for a frequently reported infectious disease.
Andy Durham
Job Title
Figure 1. Severe purulent nasal discharge increasing after internal rupture of retropharyngeal lymph node.
Strangles is an ever-present concern to the equine industry, with many hundreds of confirmed cases annually in the UK and some suggestion of a significant increase in 2025.
Strangles remains non-notifiable and control within the UK still depends on voluntary testing and management restrictions by owners of suspected cases. The Surveillance of Equine Strangles (SES) network provides useful surveillance report updates on the current UK situation.
Although high-risk scenarios exist, such as feral pony sales, it is clear that strangles may affect horses from all disciplines and backgrounds, with a recent study highlighting international transport of competition and sports horses as an important means of global spread1.
Acute strangles begins with nasopharyngeal infection, with Streptococcus equi subspecies equi (Strep equi) causing typical early signs of fever, dullness and poor appetite. The organism is unlikely to survive longer than a few days in the environment2, with the exception of water troughs, where it may persist for as long as a month in winter3. As a result, infection generally occurs following direct or indirect contact with another infected horse.
After invading the nasopharyngeal mucosa Strep equi may then colonise local lymph nodes causing lymphadenopathy and, frequently, abscessation, which defines the condition. Common infection sites include the submandibular and parotid lymph nodes, which tend to rupture externally, and the retropharyngeal lymph nodes, which tend to rupture internally through the floor of the medial compartment of the guttural pouches. Although nasal discharge may occur during the early nasopharyngeal infection, the most profuse purulent discharge tends to follow rupture of abscessated lymph nodes (Figure 1).
Although many infectious respiratory diseases affect horses in the UK, none are reported with anything like the frequency of strangles, meaning that the latter should be foremost in the mind of the clinician when faced with a horse showing signs of fever and respiratory disease.
In 2025, more than 800 laboratory diagnoses of strangles infection were made in the UK, in contrast with less than 100 for all respiratory viruses combined. A highly important factor that should alert the clinician to a possible diagnosis of acute strangles is the absence of coughing when faced with a suspected respiratory infection. Persistent coughing is rare in strangles cases and typically reported in only 2% to 3% of cases. This contrasts markedly with its frequent presence in other respiratory infections seen in the UK, such as influenza, herpesviruses and rhinitis viruses.
Coughing associated with eating might be more common in strangles cases associated with pharyngeal discomfort and dysfunction caused by the acute infection, although coughing at other times is rarely seen.
Unfortunately, diagnostic confusion might arise due to atypical presentation, probably associated with partial immunity and/or less virulent strains. During an outbreak of strangles, a range of responses to infection will be seen, including typical acute strangles as already described, but also apparent resistance to infection as a result of previous immunity. Clearly, some horses will respond somewhere between these ends of the spectrum, with mild signs such as minimal fever, non-abscessating lympadenopathy and mild nasal discharge that might not lead to suspicion of strangles in circumstances where they were not part of a recognised outbreak.
The choice of diagnostic test for strangles confirmation may cause confusion. When faced with a suspected acute strangles case, guttural pouch sampling is not relevant, as the guttural pouch might not be involved in the disease process unless, and until, a retropharyngeal lymph node ruptures into it.
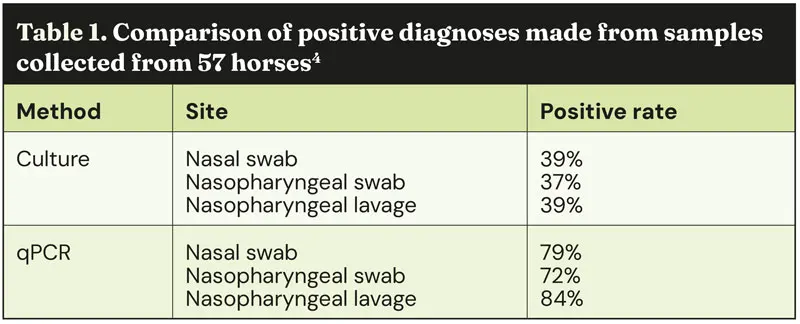
The diagnostic test of choice at an acute stage is a nasopharyngeal lavage submitted for qPCR. One Swedish study compared the diagnostic rate among 57 horses involved in 8 outbreaks of strangles (Table 1)4. The study found that qPCR detected 1.5 times as many positive cases compared to standard culture. The single best diagnostic approach was nasopharyngeal lavage subject to qPCR, and this detected 48 of 57 (84%) of cases. Collecting and submitting two samples, including both a nasopharyngeal lavage and either a nasal or nasopharyngeal swab, maximised the diagnostic rate and detected 53 out of 57 (93%) cases.
Traditionally, nasopharyngeal washes have not been used commonly in the UK, although they may clearly add to the diagnostic rate in acute strangles cases. The method is simple and involves inserting a soft plastic tube (for example, 8mm diameter, 50cm long) through one or both nares and instilling 50ml to 60ml of sterile saline (Figure 2). The saline can then be collected into a container or a sterile glove as the fluid exits the nostril. The success of this method is probably associated with sampling a much larger surface area of nasopharyngeal mucosa than a simple nasal or nasopharyngeal swab.

Treatment of acute strangles cases is generally largely supportive and symptomatic. NSAIDs are useful in controlling fever and discomfort, and are often the only medical approach required. Cleaning the sites of discharge (abscesses and nostrils) and applying barrier creams is useful, as well as closely monitoring appetite and water intake.
If isolation can be maintained, then turnout to pasture helps well-being, although longer-term contamination of water troughs should be considered, as previously mentioned. The organism is unlikely to survive on pasture for more than a few days – especially in dry or warm weather.
The issue of antimicrobial use in acute strangles cases has been regarded as contentious, although it does not differ from standard antimicrobial practice in other related circumstances.
The preferred approach for conditions involving abscesses, including strangles, is to encourage rupture and external drainage of pus, rather than using antimicrobials that often fail or just suppress infection temporarily. This is the same approach we would use for a hoof abscess or an injection site abscess, for example, and applies equally to acute strangles cases. However, in cases that appear especially sick, and where their welfare is causing concern, antimicrobials might then be indicated, just as they might for a hoof abscess that has not improved over a week or two and is causing ongoing pain and significant limb swelling.
A further scenario where antimicrobial therapy might be considered is as a preventive measure in the face of an outbreak. This is unlikely to be practical or successful if the horse remains on the affected premises due to the required duration of treatment, although it might be considered temporarily where a horse is being removed from the affected premises to a safe and distant isolation facility. In these rare instances where antimicrobials are to be considered, then procaine penicillin is invariably first choice, as resistance is very rare and minimum inhibitory concentrations are invariably very low.
Trimethoprim-sulphonamide combinations often fail in vivo despite reasonable in vitro prediction of efficacy. Tetracyclines are successful in most, but not all, cases and would be a reasonable choice where procaine penicillin is impractical depending on in vitro sensitivity results. As previously mentioned, acute strangles is a nasopharyngeal infection that often leads to local lymph node infection. In some, but not all, subacute cases the retropharyngeal lymph nodes abscessate and rupture into the guttural pouch that lies immediately dorsally (Figure 3).

A guttural pouch empyema then follows that will be successfully cleared in most cases via drainage into the nasopharynx, although this may take several weeks. However, a proportion of those horses affected by guttural pouch empyema will fail to clear infection, resulting in persistence of infective material in one or both guttural pouches.
Although some have suggested the prevalence of persistent silent carriers to be around 10%, published evidence suggests the actual figure is far lower, and most likely in the region of 2% to 3%3,5. In the latest strangles cases, the infection is likely to be purulent, but then inspissates over time and is most frequently encountered as a semi-dry crumbly material similar in consistency to cottage cheese. If further dehydration continues over time, then eventually hard discrete chondroids may form, although this probably takes months or years.
Occasionally, guttural pouches are encountered that appear visually normal without evidence of infection, although nevertheless retain Strep equi infection. Guttural pouch empyema can be flushed out successfully via an indwelling Foley catheter placed via the ipsilateral nostril.
Firm chondroids can also be removed successfully, if sometimes laboriously, via an endoscope and basket forceps. However, crumbly semi-inspissated pus presents greater difficulty with removal, and sometimes rehydration of the pus associated with frequent flushing through a Foley catheter helps removal, otherwise surgical approaches should be considered.
When faced with a guttural pouch that appears visually “clean” but is positive by qPCR, then deposition of sodium penicillin into the pouch is generally successful in removing residual bacteria. Although mixing penicillin with gelatin or poloxamer gel has been advocated by some, no evidence exists to suggest any better response than with far simpler sodium penicillin dissolved in water or saline, which seems highly effective.
Occasional cases are encountered where infection persists despite local treatment of the guttural pouch. In these cases, a careful re-examination of the guttural pouch is important. Often a small fragment of pus might be seen somewhere in the pouch, or alternatively a granulating fistula from the subjacent retropharyngeal lymph node, suggesting intermittent discharge and reinfection is still taking place. Rarely, frustrating cases are seen where infection persists despite no evidence of other guttural pouch pathology. One must then consider persistent infection at another site, such as a sinus causing reinfection via the nasopharyngeal ostium.
An historical myth that continues to cause problems in the profession is the suggestion that Strep equi serology can indicate the likelihood of guttural pouch infection. This has never been demonstrated in peer-reviewed publications despite having been strongly advocated and made popular several years ago.
Indeed, a study from 2008 showed that although acute strangles cases mount a detectable antibody response, this waned at a similar rate regardless of whether horses become carriers thereafter6. It would, therefore, appear that the equine immune system “ignores” Strep equi harboured within the guttural pouch, at least based on all serologic tests used to date. Unfortunately, in practice we are still asked frequently to perform such serologic tests to establish absence of infection pre-movement, despite this having no scientific basis. In fact, one study indicated a greater likelihood of sero-negativity in guttural pouch carriers7.
Identification and treatment approaches to strangles cases depends on the suspected stage of infection. Acute cases are best diagnosed via qPCR of nasopharyngeal lavages and treatment is largely supportive. Chronic carriers are best identified via endoscopy and qPCR of guttural pouch lavages, and treatment involves physical clearance followed by local penicillin instillation.
Andy Durham qualified from the University of Bristol in 1988 and worked initially in the midlands, where he gained a postgraduate qualification in equine practice before joining Liphook Equine Hospital in 1994. After a brief period away, he returned to Liphook in 1999 and became a partner in 2001. He gained the RCVS Diploma of Equine Internal Medicine in 2003 and the Diploma of the European College of Equine Internal Medicine the following year. Andy is also a visiting professor at the University of Surrey and acts as a consultant for internal medicine, providing a referral service for referring vets, and runs the diagnostic laboratory at Liphook. He has more than 90 peer-reviewed publications and textbook chapters on a wide range of equine medicine subjects, and lectures frequently both in the UK and abroad.