5 Dec 2016
Elisabetta Mancinelli takes a closer look at this condition and how it can be diagnosed, as well as suggesting various treatments.
Elisabetta Mancinelli
Job Title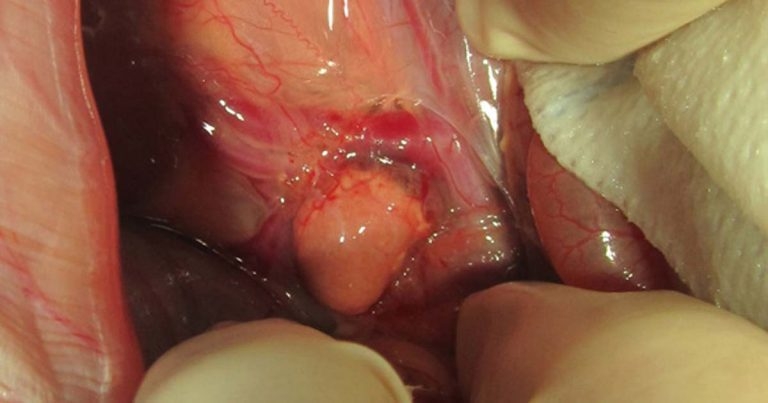
Figure 1. Gross appearance of abnormal left adrenal gland during exploratory laparotomy.
A neutered male, crossbreed domestic rabbit, of unknown age, was presented for chronic weight loss and persistent sexual behaviour.

The rabbit had been neutered at a young age and recently rehomed with its female partner due to urine spraying, loss of litter training, chinning, aggression towards and humping of his companion, the cat, the pet chicken and other members of the family.
The referring vet had taken a blood sample and performed an exploratory laparotomy. Haemato-biochemistry results were within normal limits and the surgery failed to identify any retained testicular tissue.
On physical examination, the rabbit was thin (bodyweight of 1.78kg and a body condition score of 2/5), with reduced muscle mass, but no other abnormalities could be detected. The owner declined any further investigations and opted for a trial therapy with a gonadotropin-releasing hormone (GnRH) agonist implant.
Three months later, the rabbit was presented again as no improvement was seen. A blood sample was collected to measure serum testosterone levels. An abdominal ultrasound was also performed, but did not reveal any major abnormalities. Testosterone levels were 1.7nmol/L, suggesting abnormally elevated levels (0.7nmol/L to 0.14nmol/L reference value; Fecteau et al, 2007). The owner elected for surgery and the rabbit was scheduled for an exploratory laparotomy to rule out an adrenal tumour or identify another possible ectopic source of testosterone. The patient was anaesthetised, intubated and aseptically prepared for surgery.
The only abnormal finding was a gross appearance of the left adrenal gland, with a dark caudal pole and small pinpoint lesions over its dorso cranial aspect (Figure 1). The right adrenal gland and the remaining abdominal organs appeared grossly normal.
The left gland was closely associated with an adjacent blood vessel (left renal vein). The adrenal mass was carefully dissected from its wall and submitted for histopathology. The rabbit recovered uneventfully from the surgery.
Medical therapy included pain management, fluid therapy and assisted feeding. The rabbit resumed normal appetite the following day and was discharged.
Histopathology revealed an adrenal cortical adenoma. One month following the procedure, the owner reported the rabbit’s behaviour had slightly improved as he was no longer chinning and spraying less, but was still mounting other animals in the house.
The rabbit died three months later, reasons were unrelated and no postmortem was performed.
The left adrenal gland lies lateral to the aorta and cranial to the left renal vein. The right gland is more cranial and located dorso lateral to the caudal vena cava, caudal to the liver and cranial to the right renal vein. This anatomical location is similar in all small exotic mammal species, but adrenal glands tend to be larger in smaller species (Reese, 2011).
The left cranial and left medial adrenal arteries from the aorta supply the left adrenal gland. The right cranial and the right caudal adrenal arteries from the abdominal aorta and the right renal artery supply the right adrenal gland (Popesko et al, 1992).

The adrenal glands cannot be seen in radiographic images of small exotic mammals (Reese and Hein, 2011). It is much easier, due to their size, to see these glands using ultrasonography.
In rabbits, the adrenal glands have an ovoid to almost round shape. They appear hypoechoic to the surrounding tissues, with an evident hyperechoic line in the middle, but not a distinct corticomedullary junction (Banzato et al, 2015). Reese (2011), reports instead, a marked distinction between the hypoechoic cortex and the echo neutral medulla. Ultrasonographic length and diameter of rabbits’ adrenal glands have been reported (Reese, 2011; Banzato et al, 2015; Table 1).
Testosterone-producing adrenal tumours have been described in several species, including humans (Lennox and Chitty, 2006).
In ferrets, the disease is well-documented and linked to early gonadectomy (Rosenthal and Wyre, 2012), but there is not much information available for rabbits (Lennox and Chitty, 2006; Lennox, 2013).
Persistent sexual and aggressive behaviour in neutered, especially older, animals are common presenting signs, linked to increased testosterone levels. Six cases have been reported so far in the literature, with an average age at diagnosis of 7.6 years. Symptoms reported included mounting and chasing (humans and other pets), biting, scratching and urinating over objects, owners or other pets (Lennox, 2013). In those cases, the right or left adrenal gland was affected by hyperplasia or neoplasia (for example, carcinoma). The diagnosis was based on a combination of history, presenting signs, elevated testosterone levels, the absence of other obvious testosterone sources and confirmed by histopathology after removal of the gland. Ultrasonography did not seem to be helpful for a definitive diagnosis (Lennox, 2013), as was in the case presented.
Beyer et al (1969), established, in normal rabbits, the adrenal glands secrete appreciable amounts of sex steroids. Most mammals also have accessory adrenal cortical tissue nodules and sex steroids may also be produced from other non-glandular tissues.
Fecteau et al (2007) reported reference ranges for testosterone and other sex hormones in neutered rabbits of both sexes. In fact, early evidence exists that other hormones (for example, progesterone) may also be altered. Based on the presented case report, and on the few cases described in the literature, surgical adrenalectomy is, so far, considered the possible preferred treatment.
The technique is similar to that described for ferrets (Lennox, 2013). Isolation and ligation of supplying vessels, followed by blunt dissection, can allow complete excision of the left gland, as in the case hereby described, where hemoclips were used. The right adrenalectomy is more challenging due to the close association of the gland with the vena cava. Lennox (2013) reports only three out of six rabbits underwent successful partial or full adrenalectomy, which led to only temporary resolution of clinical signs.
In the author’s case, complete excision of the left adrenal gland was performed, but this resulted only in partial improvement of the symptoms reported.
Hormonal therapies attempted in some of the reported cases, alone or in combination with surgery, included leuprolide acetate, flutamide, trilostane and deslorelin. The response was variable.
In a study, application of a slow-release GnRH agonist implant did not reduce testosterone concentrations, nor affected spermatogenesis, in treated New Zealand white rabbits. The authors concluded such an implant did not induce hormonal castration in male rabbits, over a period of 90 days, indicating it is not a suitable alternative to surgical castration in this species (Goericke-Pesch et al, 2015).
The prognosis for adrenal gland disease in rabbits remains uncertain due to the low number of cases reported. For the same reason, specific indications on the best approach cannot be given.
Elisabetta Mancinelli
Job Title