15 Jul 2019
Paddy Gordon discusses how to effectively prevent disease through good management, housing and nutrition.
Paddy Gordon
Job Title
Image: © Scott Latham / Adobe Stock

Readers of Vet Times may have read my December 2018 article on minimising ketosis. This covered how to recognise ketosis using milk or blood tests, the clinical presentations that result from this gateway disease and how to reduce the risk of ketosis through improved farm management, with a case example.
This article shifts attention from the adverse outcome of ketosis, to disease prevention through good management, housing and nutrition. While ketosis is a major consideration, other diseases that impact on health and production need consideration, too, and include milk fever, metritis, mastitis and displaced abomasums.
The preceding early dry period needs consideration to ensure a successful transition period. Cows should be dried off in appropriate body condition of 3 to 3.5. A range will always exist, so the expectation is 80% of cows will fit this target. Farms with health and fertility issues will often end up with a high proportion of outliers, with lameness and Johne’s disease resulting in poor body condition, while poor fertility often results in overfat cows due to extended lactations.
Individual lame cows must be effectively treated prior to the onset of the next lactation, when intake and energy requirements will increase. Routine foot trimming usually takes place at dry off, but it is important this both effectively treats any lameness and trims the claw in preparation for the following lactation.
Routine treatments will have been administered, and this will include dry cow therapy, vaccinations and possibly trace element boluses. Dry cow therapy should always include internal sealants, as this will reduce the risk of new infections in the dry period. Some milk contracts preclude use, but in general, both high and increasing uptake exists.
Increasing adoption of selective dry cow therapy also exists, reducing the use of dry cow antibiotic treatments, which are only required where a history of elevated somatic cell counts and mastitis is present. Critical aspects are correct selection and appropriate hygiene at drying off.
Vaccination is most commonly for stimulation of maternal antibodies to provide passive immunity for calves against calf diarrhoea. Dam vaccination usually takes place at drying off.
Some farms will administer other vaccines, including Salmonella and respiratory vaccines on a risk basis, but low uptake exists in the UK. Trace element boluses can be needed where farms are reliant on forage only, or particular deficiencies exist, with iodine, selenium and copper all associated with clinical disease.
Individual cows at risk of ketosis can be identified at drying off. This can be a convenient time if pregnancy checks by the vet occur, as body condition scoring at the same time allows susceptible cows to be identified. Cows are not treated at that time, but are spray marked or tail taped to allow treatment three weeks before calving. Alternatively, the farmer may identify susceptible cows at drying off.
Nutritional requirements are to feed a so-called “Goldilocks diet”, indicating not too much and not too little of the key ingredients of energy, protein and fibre. Far-off dry cow diets should be high fibre and low energy, and this can be achieved with low-quality grazing, conserved forages (round bale silage or grass silage and straw mix) or a mixed ration. As always, the devil is in the detail, with farmer and nutritionist able to formulate and deliver an appropriate ration that is freely available and avoids sorting.
Liam Sinclair at Harper Adams University, in a survey of 50 farms throughout the UK, found poorly mixed rations on 58% and sorting on 66%.
A total of 34% of the herds were feeding for zero refusals, which is a real concern as animals low in the pecking order (such as heifers and lame cows) are then likely to suffer restricted intakes.
Farms will typically move cows to grazing or sheds close to the dairy, where they can be more closely observed for calving. The timing of this move is critical, and should be three weeks prior to calving for cows and at least this for heifers. Feed intakes are likely to reduce around the time of any move, and movement close to calving (less than 19 days) can impact on health. Sufficient feed space is needed at this time of at least 75cm, and ideally 1m, and 10cm water trough length per cow. While this may be planned for, based on average numbers calving, fluctuations in fertility will often mean periods occur when these targets are not achieved. Housing should be planned for a 40% variation in numbers (20% above and 20% below average).
Diets for the close-up dry cows may be the same as for the far-off dry cows, or a higher energy diet may be fed to prepare cows for the milking ration. Close-up group target feed intakes are around 12kg to 15kg dry matter, target energy intakes are around 120MJ and a dietary protein content of 13% to 14%.
The presentation and access to the diet – with no spoilage, feed pushed up frequently and feed access unrestricted – are essential aspects. Monitoring intakes is essential as changes in body condition will not be apparent during the short time cows are in this group. Faecal consistency can be used to judge ration balance, but better still is to assess non-esterified fatty acids (NEFAs) in this group.
Oetzel recommended 90% of cows at 2 to 14 days precalving should have NEFAs less than 0.4mEq/L, with 12 animals tested. Elevated NEFAs indicate dry cow housing, management and nutrition need attention as cows are mobilising body fat prior to calving.
As indicated in the author’s previous article, ensuring cows are in good health and body condition is crucial. At-risk cows need support and targeted Kexxtone bolus administration can minimise the number of cows affected by periparturient disease due to underlying ketosis.

A key aspect of close-up transition cow feeding is control of hypocalcaemia. Keeping this group separate from far-off dry cows allows targeted mineral supplementation, reducing risk and cost. The traditional UK approach has been magnesium supplementation using calcined magnesite (magnesium oxide) or magnesium chloride, delivering 20g to 25g magnesium. Magnesium can be fed via the water supply for grazed animals or via a mixed ration.
Grazing can achieve satisfactory outcomes with herds at moderate production levels, where the grass is of lower quality (so-called standing hay) and adequate intakes of magnesium supplementation exist. This is more difficult to achieve in a wet year where good grass growth occurs.
Other approaches exist, including dietary cation-anion balance (DCAB) manipulation or calcium restriction. The mineral balance is altered to achieve a partial metabolic acidosis with DCAB diets. In practice, this means the addition of chloride ions (often as magnesium chloride, but also magnesium sulphate and ammonium chloride) while restricting intakes of sodium and potassium. DCAB diets are best fed as a mixed ration as these salts are unpalatable.
Some herds can feed DCAB rations at grazing and, in these circumstances, it is essential for the cows to be eating adequate fed ration as this contains the mineral supplementation. A minimum of 7kg on a dry matter basis of the supplemented ration should be achieved. Housed periods allow greatest control of intakes and ration.
Outcomes can be assessed on the basis of clinical milk fever incidence, and this should always be less than 5%. Urine pH monitoring can be used with DCAB diets and an acidic urine pH 5.5 to 6.5 should be achieved.
Alternatively, blood samples can be taken between 12 and 24 hours after calving. This requires training of farm staff in blood sampling technique. Testing primiparous animals is not needed and 12 animals are required to build up an adequate picture. The alarm level is 30% of animals should not fall below 2mmol/L calcium.
Milk fever can be a costly disease, as an unresponsive clinical case can progress to a downer cow with risk of culling. Subclinical milk fever will also occur, and this can manifest itself as uterine inertia and cows slow to calve, or as retained fetal membranes and metritis, and left displaced abomasum.
Assessment of the level of subclinical hypocalcaemia is worthwhile, as it may be unrecognised, and health and production benefits are likely to occur from addressing this condition. A study by Reinhardt of nearly 1,500 cows found subclinical hypocalcaemia incidence may be as high as 50% in cows from second lactation.
While diet change will be used to minimise milk fever risk, some animals at higher risk are likely. These are older, high-yielding cows, but also fat cows, twin calvings and lame cows. Calcium supplementation at calving can be used in these cows or during high-risk periods.
Calcium boluses are given at the time of calving and again 12 hours later. The aim is to help the cow achieve physiological levels of calcium, and should not be used to treat clinical milk fever. Oetzel and Miller found calcium supplementation at calving in above average and lame cows resulted in additional yields, even where low levels of subclinical hypocalcaemia were present.
A 180-cow robotic dairy asked for help in improving farm fertility. The farm had impressive fertility performance, with InterHerd+ figures of 46% pregnant at 100 days after calving, calving to first service interval of 63 days and 21% of cows eligible for service conceived. A farm visit found further attention to transition cow management and fertility protocols had the potential to maintain or improve fertility, improve health and increase milk production levels.
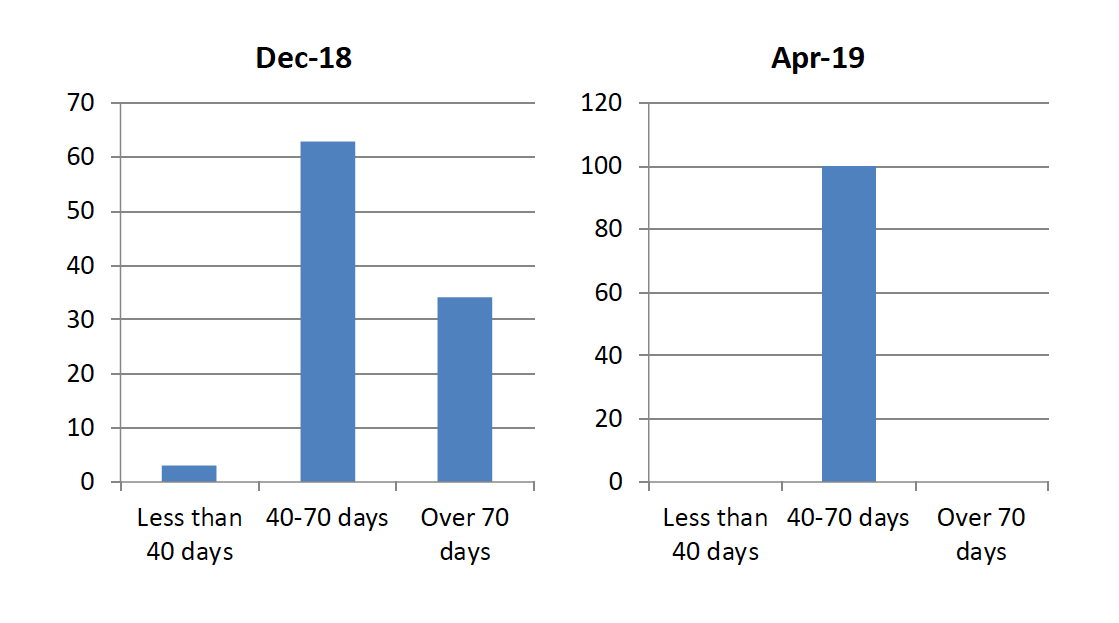
Dry period length of 72 days was too long, and would have increased the risk of cows gaining body condition while dry and being overfat at calving. A target dry period of 56 days was set, with more than 80% of cows to have a dry period length of 40 to 70 days.
This issue had come about because of retaining and rebreeding long lactation cows to populate the herd during a period of herd expansion. Cows with long dry periods, as well as older or fat cows, were to be given Kexxtone boluses prior to calving.
Advice on dry cow diets were as follows. Dry cow diet chop length was found to be long, and advice was given to chop further to reduce the risk of sorting. The feed face was to be cleaned every other day to ensure clean feed presented and prevent intakes being affected by feed spoilage.
It was ensured adequate feed space of at least 75cm was achieved by correct grouping of cows. As all cows were on the same dry cow diet, moving cows to a transition group was less critical. Dry cow intakes were to be monitored to ensure reaching a minimum of 12kg dry matter.
Every cow was assessed for ketosis at day four after calving. Testing was to be carried out by the herdsman using a blood glucose and ketone monitoring system. Cows with a β-hydroxybutyrate level greater than 1mmol/L were to be given 300ml oral propylene glycol daily for three days, and their health and production closely monitored.
The herd was assessed for subclinical hypocalcaemia by blood testing cows in third lactation and above on day of calving. Initial testing on a small sample identified subclinical hypocalcaemia to be an issue.
Fertility protocols were altered to extend the voluntary wait period to 50 days from 42 days. This was due to evidence that lifetime milk yield can be lost from short lactations – especially in younger animals. This approach is only recommended where herds have high heat detection rates. Cows not observed in heat were to be presented to the vet at an average of 63 days.
Cows not in calf, nor responding to prostaglandin treatments, were to be put on a controlled internal drug release-synch regime to maximise pregnancy rate. These pregnancy diagnosis negative cows that have not been rebred were at increased risk of culling as their days in milk approach the cut-off for breeding of 220 days. Fertility outcomes were to be monitored on a regular basis using pregnancy rate.
Initial results showed a ketosis level typical of UK dairy herds of 28%, with 28% of cows also showing some clinical disease after calving. Clinical presentations included milk fever, retained fetal membranes and metritis.
This has increased awareness of disease levels – both clinical and subclinical – and increased recognition that the potential exists to manage both the herd and individuals to optimise health and fertility.
Calving is the most critical time in a dairy cow’s production cycle. Common underlying causes exist to many of the clinical diseases seen, and these can be prevented in most animals with good housing, management and nutrition.
Individuals at greater risk will still exist, and recognition of these and targeted preventive treatments will help reduce disease incidence further. Putting in place systems to monitor metabolic health and treat susceptible individuals can help transform health, production and fertility.