9 Jun 2020
Cristina Toni and Sebastien Behr discuss Prince – a five-year-old male, castrated Staffordshire bull terrier – in this Case Notes from <em>Vet Times</em>.
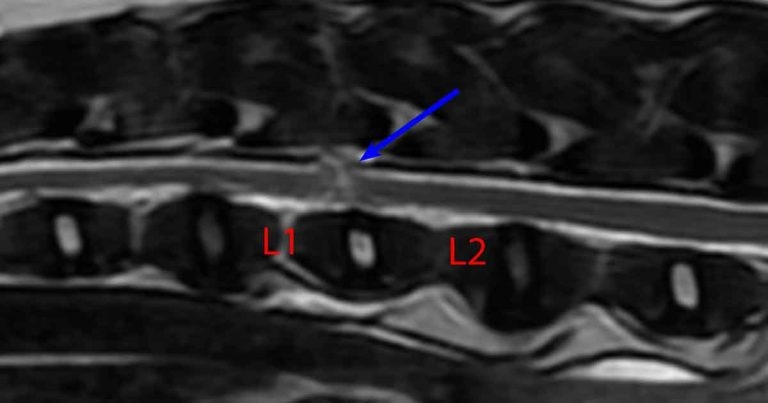
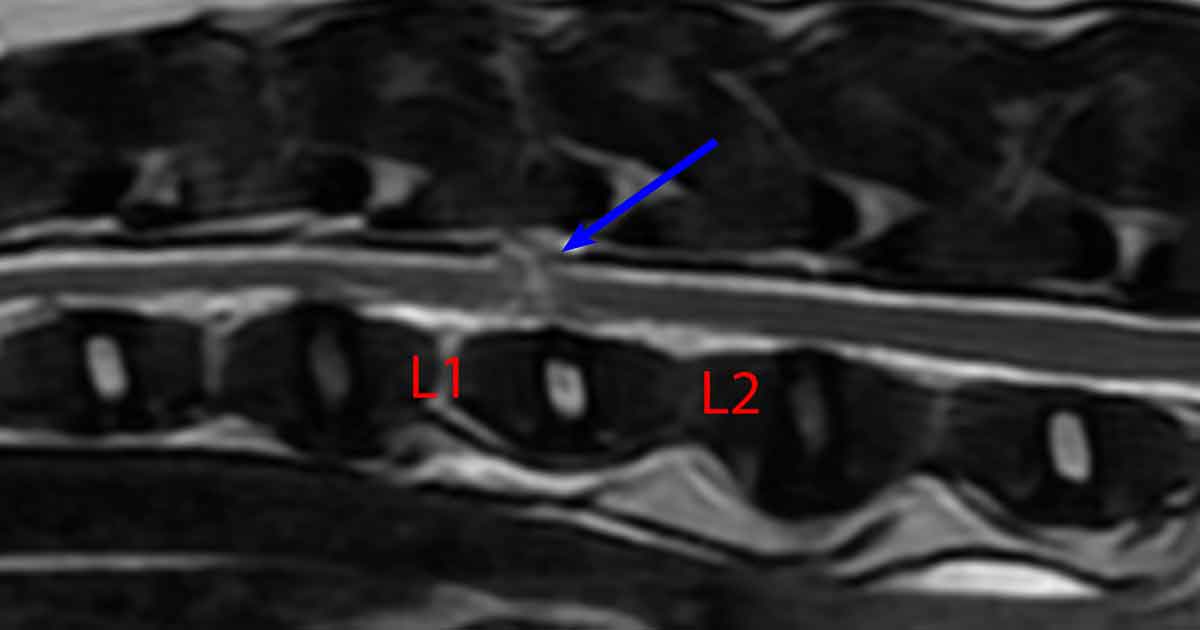
T2-weighted MRI sagittal view showing the acute lesion of the spinal cord between L1 and L2 (blue arrow).
At the beginning of an out-of-hours shift, Prince – a five-year-old male, castrated Staffordshire bull terrier – presents to you unable to walk on his pelvic limbs.
The owners reported he was chasing a cat, when he yelped and immediately appeared “paralysed” on his hindlegs.
General physical examination is unremarkable. Neurological examination reveals a severe non-ambulatory paraparesis in his pelvic limbs, worse in the left pelvic limb.
Segmental spinal reflexes are intact and Prince has good nociception in both pelvic limbs. No spinal pain exists on palpation of the vertebral column. The cutaneous trunci reflex is cut off at L3 on both sides and thoracic limbs examination is within normal range. Cranial nerves examination is unremarkable.
Based on the aforementioned findings (upper motor neuron signs in both the pelvic limbs), a T3 to L3 spinal cord segmental anatomic diagnosis is suspected.
Based on the history and examination of a hyperacute, non-progressive and non-painful T3 to L3 lesion, the main differentials would be a vascular event, such as an ischaemic myelopathy (also called fibrocartilaginous embolism), an acute non-compressive nucleus pulposus extrusion (ANNPE) and, less likely, an acute disc extrusion (Hansen type-one disc herniation).
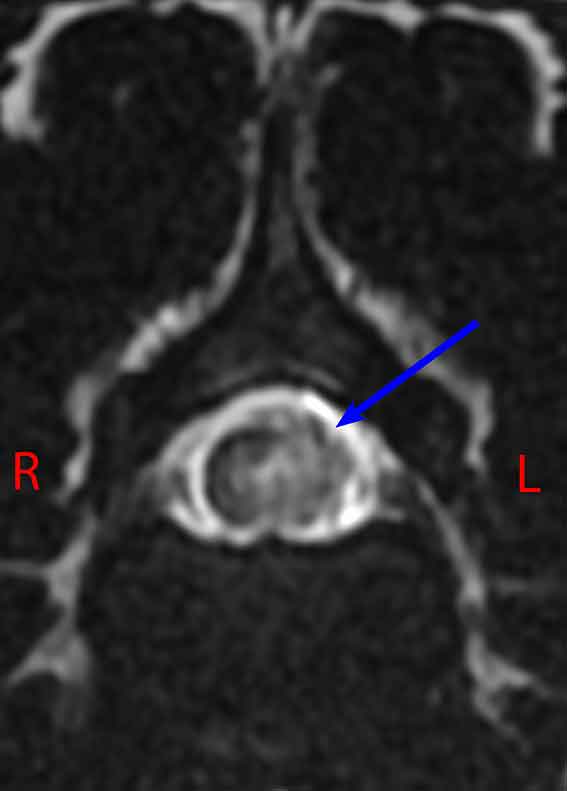
Based on these likely differentials, an MRI study of the thoracolumbar spine is recommended. This reveals an L1 to L2 non-compressive hydrated nucleus pulposus extrusion with focal left-sided myelopathy (likely oedema). Mild non-compressive extradural haemorrhage is also noted.
What would be your recommendations for treatment and how would you advise the owners with regard to prognosis?
The magnetic resonance revealed an ANNPE. An ANNPE is where a hydrated nucleus pulposus extrusion occurs into the spinal canal – usually as a result of a rapid increase in intradiscal pressure secondary to either trauma or strenuous exercise (De Risio et al, 2009).
The hydrated disc is thought to extrude through a tear in the annulus fibrosus. The latter usually occurs with significant velocity, when this material makes contact with the spinal cord, and a significant concussive damage can occur.
As the nucleus is hydrated, it tends to dissipate throughout the epidural space – hence the lack of a residual compressive lesion. As no significant compressive lesion exists, surgery is not beneficial in these cases and surgical management is, therefore, not indicated.
Treatment is supportive and, depending on the degree of neurological impairment, may consist of a combination of nursing care, physiotherapy and hydrotherapy. Analgesia – in the form of NSAIDs and other analgesia medications – are indicated if the patient has back pain (De Risio, 2015).
Clinical outcomes of dogs with presumptive ANNPE have previously been investigated with successful functional recovery (defined as recovery of unassisted ambulation and complete urinary/faecal continence) in 66.6% of dogs (De Risio et al, 2009).
In a study comparing fibrocartilaginous embolic myelopathy (FCEM) versus ANNPE, ambulatory function was regained in 99% of cases, with persistent motor deficits in 83.6% and 92.5% of dogs with presumptive ANNPE and FCEM, respectively.
Faecal incontinence was five times more likely in dogs with presumptive ANNPE (23 per cent) compared with presumptive FCEM (7.5%; Mari et al, 2017).
Prince was hospitalised for 48 hours to manage his pain and monitor for any further deterioration. He was treated with meloxicam 0.1mg/kg once daily.
Prince was discharged 48 hours after admission. At the time of discharge he had good voluntary movement in the right pelvic limb and still minimal movement in the left pelvic limb. A course of meloxicam 0.1mg/kg oral solution to be given once daily for 10 days – and gabapentin 10mg/kg oral capsule three times a day for 14 days – were recommended to the owners.
The owners were shown how to perform physiotherapy, which they performed three to four times daily. Finally, the owners were advised to strictly rest Prince when not under direct supervision.
A month following admission, Prince had a really satisfactory recovery from his ANNPE. He was ambulatory with a mild postural deficit on his left pelvic limb.
ANNPE should always be considered as a possible differential in all non‑chondrodystrophic dogs presented with a peracute onset of a transverse myelopathy – especially if associated with exercise and neurological signs compatible with spinal disease.