23 Jul 2018
Marge Chandler discusses dietary management of senior small animals and provides advice practitioners can give to owners.
Marge Chandler
Job Title
Figure 1. An older dog showing a greying of the muzzle. Image: Julie Churchill
An increase in the percentage of elderly pets has occurred, similar to humans. About one-third of pet dogs and cats in the UK are more than seven years of age, although the age a pet becomes “old” is difficult to define and old age is not a disease.
The median age of death for cats and dogs in the UK is 14 and 12 years, respectively (O’Neill et al, 2013; 2015). The longest-lived dog breeds in this survey were the miniature poodle, bearded collie, border collie and miniature dachshund, while the shortest lived were the dogue de Bordeaux and great Dane. The size of a dog affects its life expectancy; small dogs generally live longer than large ones. The popularity of smaller dogs has increased in recent years, although as some of these are brachycephalic breeds their lives may be shortened by related disorders.
In a UK study, cross-bred cats had a higher median longevity than purebred cats (median 14 years versus median 12.5 years), but individual purebred cat breeds varied substantially in longevity (O’Neill et al, 2015). A breed difference existed for purebred cats; for example, Siamese live longer and Persians tend to have shorter lives than other breeds.
The leading non-accidental (non-trauma) causes of death in dogs and cats are cancer, kidney disease and heart disease, and in cats also hyperthyroidism. A dog or cat may be considered geriatric during the final third of its expected life. Adult cat ages have been divided into “adult” (from 1 to 11 years of age), “senior” (from about 11 to 14 years) and “geriatric” (more than 15 years). The year when a dog or cat is senior or geriatric should be determined more based on physiological changes associated with ageing, such as decreased mobility and greying of the coat rather than a chronological age (Figure 1).
Anti-ageing strategies should focus on the areas where intervention may have an effect not only on length, but also on quality of life, such as decreasing intracellular damage by free radicals, improving mobility, improving cognition and dental health.

An age-associated change occurs in body composition in humans, cats and dogs, with a loss of lean body tissue and an increase in the relative percentage of fat. Loss of muscle mass is termed sarcopenia.
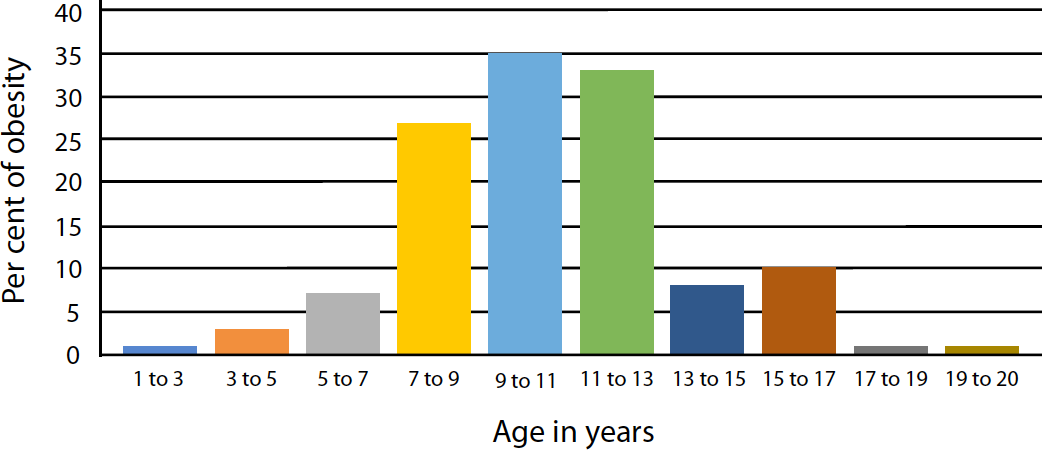
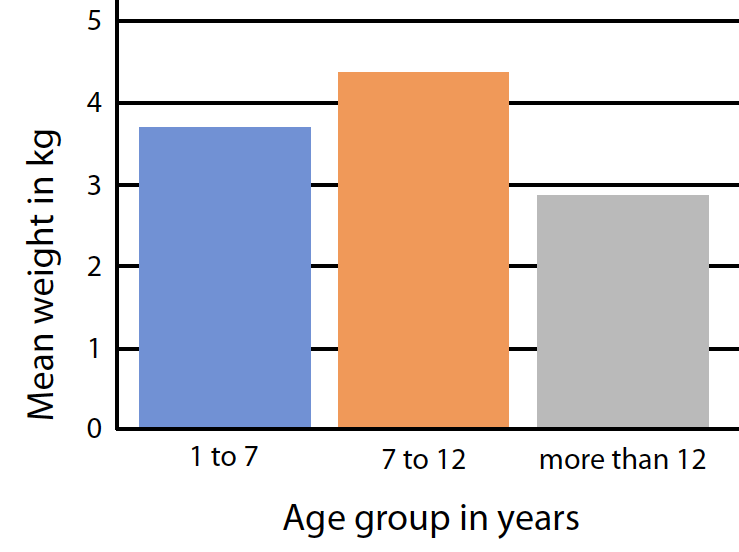
The average cat gains bodyweight steadily from 1 year of age to about 7 years of age, but after 12 years of age may tend to lose weight. The incidence of obesity is, therefore, highest at middle age and is estimated to affect one-third or more of cats (Figure 2). In geriatric cats more than 12 years, fat and lean tissue, as well as bodyweight, decreases (Figure 3). By 15 years, cats have a mean lean tissue value of less than 2kg; one-third less than the mean of 3kg during adult stage. The speed of decline appears to be a predictor of the time of death (Perez-Camargo, 2010; Williams, 2018).
In humans, the loss of muscle mass is thought to be due to reduced physical activity, ageing of the CNS, loss of motor units, and decreased circulating growth hormone, testosterone and oestradiol. An additional contributing cause can be an inadequate intake of energy and/or protein, and many older cats may have an enteropathy that causes malabsorption of nutrients (Williams, 2018).
Elderly humans have a reduction in the number of taste buds, leading to a relative preponderance of bitter and sweet receptors. Food previously enjoyed may taste bland.
Older pets are similarly thought to have a decreased ability to smell and taste (Fascetti and Delaney, 2012; Fortney, 2010). A decrease in saliva production can also contribute to a decreased appetite. Older dogs may be more likely to only eat a single food and many cats seem to want a variety of foods. Enhancement of flavours or food added to the pet food may encourage appetite in older pets, although added foods should be limited to 10% or less of the caloric intake so the diet does not become deficient or unbalanced (Figure 4; Table 1).
Elderly humans have slowed gastric emptying and reach satiety sooner than younger people, so they benefit from frequent small meals. It is likely elderly pets, especially cats that normally prefer to eat multiple small meals, would also benefit. When allowed and available, older cats eat 12 to 14 meals per day, compared to young cats that eat 11 to 12 meals per day.

| Table 1. A comparison of canned tuna for humans with the nutrient requirements of adult cats. Only bars in green show nutrient values that fulfil European Pet Food Industry Federation (FEDIA) nutrient requirements | ||||
|---|---|---|---|---|
| Nutrients | FEDIA requirement | Percentage of requirement | Amount (per Mcal) | Requirement range |
| Phenylalanine | 628.1 | 7.223g | 1.5g to no limit | |
| Phenylalanine-tyrosine | 306.1 | 13.467g | 4.4g to no limit | |
| Taurine | 0 | 0g | 0.5g to no limit | |
| Threonine | 540.5 | 8.108g | 1.5g to no limit | |
| Tryptophan | 561.1 | 2.076g | 0.37g to no limit | |
| Valine | 648.6 | 9.534g | 1.47g to no limit | |
| Total lipid (fat) | 103.4 | 23.267g | 22.5g to no limit | |
| 18:2 undifferentiated | 34.5 | 0.431g | 1.25g to no limit | |
| 20:4 undifferentiated | 2663.6 | 0.4g | 0.015g to no limit | |
| Carbohydrate | 0 | 0g | 0g to no limit | |
| Biotin | 0 | 0mg | 0.019mg to no limit | |
| Choline | 39.5 | 229.54mg | 581.077mg to no limit | |
| Folate | 7.8 | 15.668mcg_DFE | 200mcg_DFE to no limit | |
| Niacin | 454.3 | 45.43mg | 10mg to no limit | |
| Pantothenic acid | 67.5 | 0.971mg | 1.44mg to no limit | |
| Riboflavin | 34.5 | 0.345mg | 1.0mg to no limit | |
| Thiamin | 4.5 | 0.063mg | 1.4mg to no limit | |
| Vitamin B-12 | 162.8 | 0.009mg | 0.006mg to no limit | |
| Vitamin B-6 | 269.8 | 1.7mg | 0.63mg to no limit | |
| Vitamin E | 70.1 | 6.659IU, Vit D | 9.5IU, Vit D to no limit | |
| Vitamin K | 78.4 | 0.02mg | 0.025mg to no limit | |
| Calcium | 7.4 | 0.11g | 1.48g to no limit | |
| Chloride | 0 | 0g | 0.29g to no limit | |
| Copper | 24.5 | 0.306mg | 1.25mg to 7.1mg | |
| Iodine | 0 | 0mg | 0.125mg to 2.8mg | |
| Iron | 38 | 7.599mg | 20mg to 355mg | |
| Magnesium | 259 | 0.259g | 0.1g to no limit | |
| Manganese | 11.9 | 0.149mg | 1.25mg to 42.6mg | |
| Phosphorus | 136 | 1.7g | 1.25g to no limit | |
| Potassium | 123.8 | 1.857g | 1.5g to no limit | |
| Selenium | 686.3 | 0.515mg | 0.075mg to 0.142mg | |
| Sodium | 1554.2 | 2.953g | 0.19g to 4.5g | |
| Zinc | 20 | 3.76mg | 18.8mg to 71mg | |
| Retinol | 18.8 | 47.005mcg | 249.9mcg to 30,000mcg | |
| Vitamin D | 1002.8 | 626.729IU, Vit D | 62.5IU, Vit D to 568IU, Vit D | |
| Water | 100 | 573.379g | 0g to no limit | |
| Figures courtesy of Balance IT, A DBA of DVM Consulting. | ||||
Dehydration is a common problem among elderly pets. Contributing factors include decreased thirst sensation, urinary and respiratory infections, mobility problems, diuretic use, diabetes mellitus and decreased urinary concentrating ability. In elderly humans without renal disease, a decrease exists in renal glomerular filtration.
Cats more than 12 years of age similarly produce a significantly larger volume of urine than younger cats, apparently due to decreased concentrating ability even without signs of renal failure (Patil and Cupp, 2010). Making sure water is easily accessible and fresh, providing several sources of water or feeding canned food may help a cat stay hydrated. Other methods for encouraging water intake include pet water fountains, tuna flavoured ice cubes, milk spiked water or adding extra water to canned food.
In ageing dogs (more than eight years old), the mean apparent digestibility coefficients for fat, protein and energy tend to be mildly, if at all, reduced compared to younger dogs (Larsen and Farcas, 2014).
In contrast, many cats have decreased protein and fat digestibility with age, especially between the ages of 12 and 15 years (Cupp et al, 2004; Perez-Camargo, 2010). More than 20% of cats older than 14 years of age have low protein digestibility (Patil and Cupp, 2010) – this probably results from reduced intestinal function, decreased gastric acid production, gastric and intestinal motility and blood flow, and pancreatic lipase activity (Perez-Camargo, 2010).
Cats’ energy requirements decrease steadily from one year old to about seven years of age, although probably less than dogs as cats’ activity decreases less. Cats’ average energy requirements are 80kcal/kg at one year and 51kcal/kg by seven years.
As noted, the prevalence of feline obesity peaks between 8 to 13 years of age (Figure 2). Calorie restriction for obese cats and dogs is important as they have an increased risk of a number of diseases or complications of diseases, including feline diabetes mellitus (insulin resistance), hepatic lipidosis, Pickwickian syndrome (increased fat around the ribs and within the thorax compromising respiration), aggravation of orthopaedic disease (such as OA), anaesthetic complications, feline lower urinary tract disease, immunoincompetence, hypertriglyceridaemia, dermatological diseases (such as skin fold pyoderma) and a shortened life.
However, as mentioned previously, old cats lose lean body tissue and fat; in one study, none of the cats more than 15 years old were able to maintain their weight (Perez-Carmago, 2010; Figure 5). The energy needs of many cats more than 12 years of age increases along with the decreased digestibility of protein and fat (Perez-Camargo, 2010). This means increased amounts of highly digestible or higher calorie foods may be needed.

A senior or other diet with caloric restriction is not appropriate for many older cats; many of the diets for older cats are not low in calories.
Feeding small meals frequently may improve intake, and many cats will compensate for decreased absorption by eating more. Other methods for improving intake include attention to dental disorders, provision of novel foods, slight warming, flavouring and to avoid putting bad tasting medications in food.
The maintenance energy requirement for dogs more than eight years old is 18% to 20% less than one-year-old dogs. This is due largely to a decrease in activity, but also to decreases in resting energy requirement (RER). Lean body tissue is more metabolically active than fat, so the decrease in lean tissue decreases the RER.
As the ability of dogs to absorb nutrients decreases little, older dogs may need fewer calories. Obesity should be prevented or corrected for dogs susceptible to many obesity-influenced disorders, especially aggravation of arthritis. The energy needs of very old dogs (more than 12 years old) have not been well studied and may increase, as do those of very old cats.
Do older animals need less protein to prevent renal disease or the “work” of the kidneys? No evidence exists that increased dietary protein causes renal disease or affects the progression of renal disease in dogs and cats. Only high amounts of dietary protein are associated with adverse clinical signs in renal disease.
Moderate amounts of dietary protein cause no ill effects in renal failure animals and are associated with a general improvement compared with either high or low protein diets. Moderate rather than high protein concentrations will decrease azotaemia. Inadequate protein contributes to loss of muscle mass, decreased immune competence, and decreased functions of the heart, lungs, endocrine system, gastrointestinal tract and liver.
As older cats are less able to digest protein they require sufficient or even extra protein. The protein requirement of cats with chronic kidney disease and healthy controls appears to be approximately 20% of the calories (Kirk and Hickman, 2000) and may be higher in geriatric cats. Highly digestible protein of good biologic value, or even hydrolysed protein diets, may benefit older cats, although studies using hydrolysed diets for geriatric cats have not been studied. The protein digestibility of dogs does not appear to decrease similar to that of cats, although it has not been researched in very old dogs. Similarly, the fat digestibility of old cats decreased, with more than 30 per cent of older cats having reduced fat digestibility (Patil and Cupp, 2010).
Strong evidence exists that dietary phosphorus should be restricted in animals with renal disease, as it contributes to high parathyroid hormone levels, which are thought to be toxic, and high phosphorus intake itself may be detrimental to the kidneys. Using phosphate binders will help decrease the amount of dietary phosphate absorbed from the diet. It is possible increased dietary phosphorus may be also injurious to the kidneys of healthy cats and excess amounts should be avoided, even in cats without overt kidney disease (Dobenecker et al, 2002).
Antioxidants are the body’s defence against free radicals (reactive oxygen species), which play a role in the ageing process and the pathogenesis of some chronic diseases. Oxidative stress may be caused by pollutants, UV light radiation, drugs, inflammation and exercise. Several nutrients act as antioxidants by trapping free radicals, including vitamins C and E, taurine, and carotenoids.
In humans, deficient intake of these can lead to suppression of immune functions and an increased incidence of infection, cardiovascular disease, cancer and arthritis. Cats fed diets supplemented with vitamin E, β-carotene, vitamin C, and lycopene and a prebiotic (chicory root) showed an enhanced humoral response to a calicivirus vaccine compared to those fed a control diet (Cupp et al, 2008). The red blood cells (RBCs) of cats on the supplemented diet were more resistant to osmotic lysis (a measure of RBC fragility) and had lower prostaglandin E2 production. The optimal doses for antioxidants in cats and dogs (or even for people) are not known.
Vitamin E has been thought to be safe; however, in a meta-analysis of humans, beta carotene, vitamin A, and vitamin E given singly or combined with other antioxidant supplements significantly increased mortality and no evidence exists that vitamin C increased longevity (Bjelakovic et al, 2007). The relevance of the data is hard to evaluate for pets, but evidence exists that, at higher doses, many antioxidants become pro-oxidants and empiric supplementation may not be as beneficial as feeding diets, where research has shown positive results.