12 Nov 2018
Mark Lowrie discusses advances of identifying and managing the various types of this condition.
Mark Lowrie
Job Title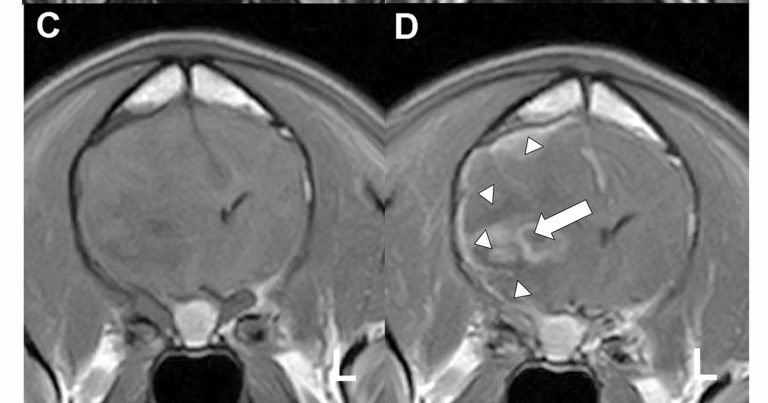
Epilepsy is defined as chronic, recurring seizures; a summary of the relevant terminology is provided in Panel 1 (Blume et al, 2001). It is not a single disease, but a group of heterogeneous disorders historically divided into idiopathic (primary) epilepsy, symptomatic (secondary) epilepsy and cryptogenic epilepsy.
Seizure: a sudden occurrence or recurrence of disease; this term is, therefore, non-specific, although it is most commonly used to describe an epileptic seizure.
Epileptic seizure: the clinical manifestation of abnormal electrical activity in the brain.
Epilepsy: epilepsy is not a specific disease, but a chronic condition characterised by recurrent epileptic seizures.
Symptomatic epilepsy is a term used to describe seizures that result from an identifiable intracranial structural lesion, such as a brain tumour, inflammatory or infectious brain disease, and congenital intracranial malformations; for example, hydrocephalus (Figure 1; Engel, 1996). Cryptogenic epilepsy describes epilepsy thought to be symptomatic, but for which the aetiology has not been determined (Engel, 2001).
Idiopathic epilepsy (IE) is a term reserved for patients with chronic, recurring seizures, but no detectable underlying abnormality; these seizures are presumed to be genetic in origin (Knowles, 1998). Importantly, this term is not applied to dogs where the cause of seizures is unknown. Instead, it refers to recognised clinical syndromes alongside typical clinical features, such as age of disease onset and a lack of other neurological abnormalities.
Epilepsy is the most common naturally occurring chronic neurological condition in dogs and estimated to occur at frequencies of 0.5% to 5.7% in the canine population (Chandler, 2006).
In some breeds, even higher prevalences have been reported; however, these figures were obtained in various studies aimed to assess seizure prevalence in specific canine breeds or referral hospital populations, which, therefore, had a potential bias towards dogs at greater risk of seizures owing to a breed predilection or concurrent medical conditions.
No study has determined the true prevalence of seizures in the general dog population. In humans, the lifetime risk of developing epilepsy is estimated to be 2% to 5%, suggesting the lifetime risk of having a single seizure is much higher (Sander and Shorvon, 1996). IE is the most common seizure disorder in dogs and diagnosed in 45% of those presented at a referral hospital for seizure disorders (Jaggy and Bernardini, 1998).
Diagnosing IE is challenging as all other possible seizure aetiologies must first be excluded. In these animals, neurological examination, haematology, biochemistry, dynamic bile acid testing, serum ammonia, MRI and CSF analysis should demonstrate no significant abnormality. First and foremost, recurrent seizures are essential for a diagnosis of IE.
Additionally, IE should be suspected in dogs that experience their first seizure between one and five years of age (Holliday, 1980). However, IE is not exclusive to this age range and some exceptions exist. For example, English springer spaniels with IE have been found to have a bimodal age distribution at onset of seizures, with peaks occurring at one to three years and five to six years of age (Patterson et al, 2005).
Occasionally, IE can start as early as at 3 months of age or as late as at 10 years of age (Jaggy and Bernardini, 1998), although some authors would describe these patients as suffering from cryptogenic epilepsy (Berendt and Gram, 1999).
As stated previously, a diagnosis of IE requires normal results of physical and neurological examinations interictally, although abnormal neurological findings may be observed in the immediate postictal period following prolonged seizures or status epilepticus. This is due to oedema that forms as a result of the acute phase of reactive astrocytosis during seizure activity (Mellema et al, 1999). If these findings are observed, it is recommended the neurological examination be repeated at least 24 hours later to ensure any neurological abnormalities are transient.
Postictal imaging abnormalities are sometimes seen on MRI during this time and appear to be reversible (Figures 2 and 3; Mellema et al, 1999).
Generalised tonic-clonic seizures were traditionally thought to be the most common seizure type in dogs with IE. However, it is widely accepted focal-onset seizures are also commonly seen in dogs with IE (Sander et al, 1996; Berendt and Gram, 1999). Indeed, the type of seizure observed does not infer a diagnosis of IE, as focal-onset seizures with or without secondary generalisation, generalised tonic-clonic seizures or any combination of these can all result from IE. Furthermore, cluster seizures and status epilepticus can also be associated with IE (Saito et al, 2001; Bateman and Parent, 1999).
The term “idiopathic” reflects the lack of understanding about the underlying aetiology. Indeed, one could argue “how is it possible to discuss the pathogenesis of an idiopathic condition?” It is accepted many dogs diagnosed with IE may not all share the same aetiology. Rather, it would seem appropriate to consider IE as a clinical syndrome with shared characteristic clinical features of potentially diverse aetiologies.
A genetic basis for IE is suspected in a number of breeds based on pedigree analysis, and a mode of inheritance has been postulated in some breeds (Table 1).
| Table 1. Canine breeds that have been shown to suffer from idiopathic epilepsy and their postulated mode of inheritance based on pedigree analysis | |
|---|---|
| Breed | Postulated mode of inheritance |
| Australian shepherd dog | Familial clustering |
| Beagle | Two forms: autosomal recessive and sex-linked suppressor |
| Belgian Tervuren | Unknown |
| Bernese mountain dog | Unknown |
| Border collie | Autosomal recessive or complex |
| English springer spaniel | Unknown |
| German shepherd dog | Unknown |
| Golden retriever | Polygenic recessive |
| Hungarian vizsla | Unknown |
| Irish wolfhound | Unknown |
| Keeshond | Unknown |
| Labrador retriever | Unknown |
| Lagotto Romagnolo | Autosomal recessive |
| Shetland sheepdog | Unknown |
| Standard poodle | Autosomal recessive |
The fact some breeds are predisposed to IE would suggest the mode of inheritance or genes may vary between breeds; however, within an individual breed, the disease is likely to be attributable to common ancestors and, therefore, the aetiology is more homogeneous (Ekenstedt et al, 2012).
Genetic studies in humans have identified an apparent association between a large number of mutations in genes that encode ion channels, neurotransmitters, or their regulatory subunits, and rare forms of IE. Some of these candidate genes have been investigated in canine IE, but similar mutations have not yet been discovered (Ekenstedt et al, 2012).
Two studies have reported genetic mutations associated with IE in dogs. The first described a mutation of the leucine-rich repeat LGI family, member 2 (LGI2) gene that occurs in the Lagotto Romagnolo breed and is responsible for a focal, remitting, juvenile-onset epilepsy (Seppälä et al, 2011). LGI2 is the first gene linked directly to a common form of childhood epilepsy in humans characterised by remission prior to adulthood. It appears to be, in part, responsible for the major remodelling of the neuronal synaptic network that occurs in the brain early in life (“pruning”).
The second report described a mutation within the ADAM23 gene associated with a high risk for epilepsy in Belgian shepherds, which is a promising finding in light of the fact ADAM23 interacts with the known epilepsy proteins LGI1 and LGI2 (Seppälä et al, 2012). However, progress in the identification of canine idiopathic epilepsy genes suggests epilepsy may represent a complex genetic disease with interaction of multiple genes and environmental factors.
Other genetic mutations responsible for other forms of canine epilepsy have been discovered. The first of these was identified in Lafora disease, a progressive, myoclonic epilepsy that occurs predominantly in miniature wirehaired dachshunds. The mutation occurs in the epilepsy, progressive myoclonus type 2B (EPM2B) gene and is a tandem repeat expansion (Lohi et al, 2005), which has implications in human medicine as this type of mutation is thought to play a role in several human neurological conditions, including Huntingdon’s disease.
A generalised photosensitive myoclonic epilepsy in young Rhodesian ridgebacks has been found to be caused by a mutation in the DIRAS1 gene that regulates acetylcholine release (Wielaender et al, 2017).
Genetic studies have developed momentum and, although the search for epilepsy genes continues, interest in identifying the genetic mechanisms of pharmacoresistance is building. Despite adequate doses and serum concentrations of standard antiepileptic drugs, such as phenobarbital and potassium bromide, up to 30% of dogs with epilepsy can develop pharmacoresistance (Schwartz-Porsche et al, 1985; Lane and Bunch, 1990).
Not only is resistance to antiepileptic drugs likely to increase the morbidity and mortality rates associated with this chronic condition, it also necessitates the development of novel antiepileptic drugs, and adds to the emotional and financial burden of the owner. The mechanisms governing pharmacoresistance have become a focus for research into canine IE (Alves et al, 2011; Weissl et al, 2012). Although drug resistance is almost certainly caused by several factors, the fact broad resistance to all antiepileptic drugs occurs in some individuals despite the different mechanisms of action of different drugs suggests drug metabolism is only part of the overall picture.
The classical hypothesis (the multi-drug transporter hypothesis) asserts altered expression of drug targets or drug transporter proteins in the blood-brain barrier (BBB) play a crucial role in chemoresistance by regulating drug transport in and out of the CNS (Löscher and Potschka, 2002). These multidrug transporters are likely to reduce the ability of antiepileptic drugs to accumulate in the brain. An example of these proteins is the permeability glycoprotein, an ATP-dependent drug efflux pump found in the BBB that can remove a large number of potentially toxic molecules from the CNS. These molecules include certain antiepileptic drugs, such as phenobarbital (Löscher and Potschka, 2002; West and Meeley, 2007).
Mutations in the ATP-binding cassette, subfamily B, member 1 (ABCB1) gene (also called the multidrug resistance 1 [MDR1] gene) that encodes this protein can result in the accumulation or excessive removal of these toxins. The authors of a study in border collies with epilepsy found a sequence variation in ABCB1 associated with drug responsiveness in this breed (Alves et al, 2011).
The multi-drug transporter theory of pharmacoresistance is only one of a number of hypotheses on the aetiology of pharmacoresistance, and pharmacogenomic investigations in humans have so far been inconclusive. A second hypothesis, known as the drug target hypothesis, has also been proposed as a potential explanation of pharmacoresistance (Kwan and Brodie, 2005). This theory asserts that intrinsic (genetic) and acquired (disease-related) alterations can occur to the structure and/or function of the antiepileptic drug targets in epileptogenic brain regions. This can lead to reduced drug efficacy. Whatever the mechanism, pharmacoresistance appears to vary between breeds, supporting the view that the genetic make-up of the patients has an influence on pharmacoresistance.
Lifelong medication is often necessary in dogs with IE. The use of the word treatment is often confusing to owners as it implies a resolution of seizures. In reality, management of seizures is the only realistic goal, and the response to antiepileptic drugs is not always satisfactory. Furthermore, antiepileptic drugs can cause transient, dose-related, or idiosyncratic side effects that may be more undesirable than the seizures themselves. The most appropriate choice of antiepileptic drug for one animal may not be the best choice for another.
When recommending any new or alternative treatment for refractory epilepsy, it is important to provide the owner with unbiased information of the expected effectiveness of the particular treatment, as well as some of the practicalities (such as the cost and frequency of dosing). Some of this information is simple and straightforward, but the major question of whether the drug is effective can be very difficult – if not impossible – to answer, as controlled studies are not available for many of the newer medications.
The majority of data on drug efficacy that will be presented in this article have been obtained from studies in which the antiepileptic drug was administered in an open-label fashion. Generally, dogs with “poorly controlled” seizures were given a novel antiepileptic drug, and seizure frequency during administration of the drug was compared with the seizure frequency at baseline.
A reduction in seizure frequency has been associated with placebo administration in dogs with epilepsy (Muñana et al, 2010). Almost 30% of the dogs in this study were classified as responders to placebo (response defined as more than or equal to 50% reduction in seizure frequency). Two reasons that may have explained this phenomenon were given.
Firstly, epilepsy is a waxing and waning disorder; therefore, normal unpredictable fluctuations in seizure frequency occur over time. Owing to the disease’s cyclical nature, an improvement in seizure frequency is likely regardless of the management regimen adopted, and this improvement may be mistakenly attributed to an instituted change in therapy.
A second factor that may play a role in this “placebo effect” is because owners enrolling their dog in a study of a novel antiepileptic drug may perceive an improvement simply through the additional attention that is provided by the investigators running the study. A study evaluating the use of anticonvulsant levetiracetam demonstrated a significant reduction in seizure frequency in all patients during the study period, independent of the treatment type (levetiracetam or placebo), as well as an improvement in owner-perceived quality of life, which supports this hypothesis (Muñana et al, 2012).
Open-label studies cannot account for this bias; therefore, the efficacy reported in the vast majority of veterinary studies of novel antiepileptic drugs may be exaggerated. The bottom line is the efficacy of many of these novel antiepileptic drugs remains uncertain, and clients should be made aware of this.
An understanding of the types of epilepsy, the classification of seizures and the benchmarks we use to define success in treating epilepsy are all vital to ensure the best possible management of a dog with epilepsy. As genetics advance it is hoped further understanding will develop, allowing catered therapeutic strategies for dogs with different types of epilepsy.