3 Mar 2026
Nicola Lakeman MSc, BSc(Hons), CertSAN CertVNECC, VTS(Nutrition), RVN discusses conditions that can impact many dogs and cats, and the underpinning knowledge required for nursing clinics.
Nicola Lakeman
Job Title
The five stages of myxomatous mitral valve disease as detailed by the American College of Veterinary Internal Medicine (ACVIM).
Cardiac disease affects approximately 10% to 15% of cats and dogs, but prevalence rises significantly with age.
This is especially the case for specific conditions like myxomatous mitral valve disease (MMVD) in dogs (up to 30% to 35% above 13 years) and hypertrophic cardiomyopathy in cats (up to 30% in older cats). This highlights the importance of nurse clinics that cater for animals with cardiac disease. Many different types of cardiac diseases are present in small animals.
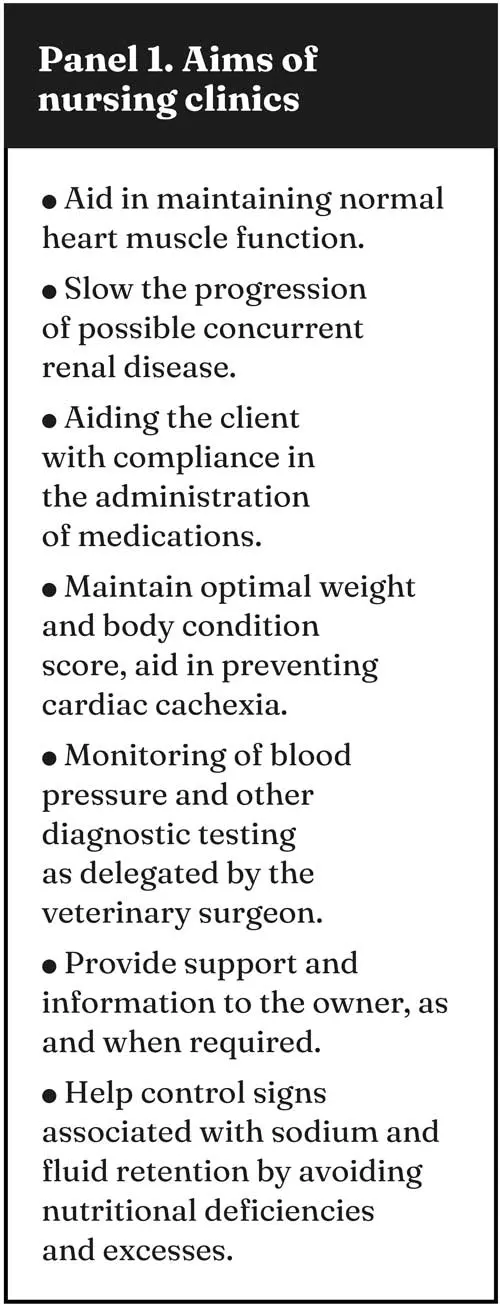
As part of the RVN clinic, the underpinning knowledge for cardiac disease is required. Panel 1 describes the aims of a nursing clinic involving an animal with cardiac disease. This includes the day one competencies of blood pressure measurement and running of an ECG trace.
The nutritional status of the cardiac patient is exceptionally important to ascertain, as this can have several effects on the patient. This can include the choice and dose rate of the drugs used in the medical treatment, interpretation of any laboratory results, interpretation of ECG data, prognosis of both surgical and medical intervention and the choice of diet for the patient.
As part of the initial clinical assessment, a full history of the animal’s diet should be taken. Nutrition can be a causative factor in cardiac disease. If the animal receives unusual supplements, is not fed a complete diet, if more than one animal in the household is affected or if it is being fed a homemade or fad diet, cardiac disease can be induced. Micro and macronutrient deficiencies (such as calcium or potassium) can cause cardiac problems, and thus a complete blood workup needs to be requested by the veterinary surgeon.
Assessment of body condition and muscle scores of each animal is required with cardiac patients. A reduction in skeletal muscle mass might indicate energy malnutrition and possibly a negative nitrogen balance. Animals with catabolic disease, such as hyperthyroidism in cats and cardiac failure, lose body mass very rapidly, as with anorexic cats.
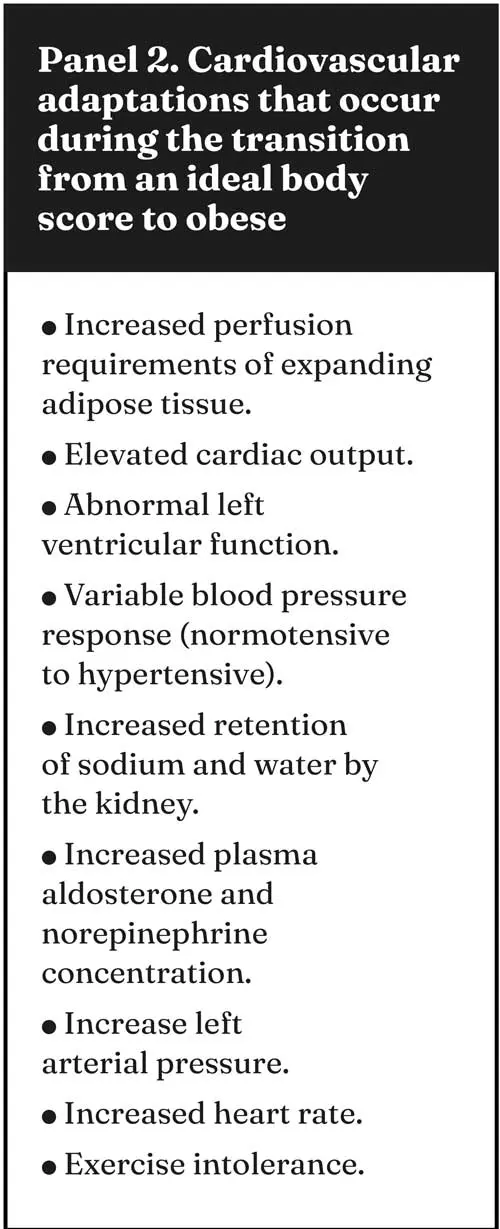
The progression of cardiac disease can be exacerbated in obese animals. This can result in cardiomegaly, circulatory congestion, oedema, ascites and hypocalcaemia. An overweight animal must be subjectively assessed; obesity must be differentiated from abdominal distension due to hepatomegaly or ascites. Obesity can also mask an underlying lean muscle body mass. Obesity not only produces clinical signs (Panel 2) that mimic those of early heart failure but can also cause cardiovascular changes that can exacerbate any underlying cardiovascular disease.
Between 34% and 75% of dogs suffering from heart disease suffer from anorexia, and it is one of the multifactorial processes associated with the loss of lean body mass in cardiac cachexia1. Other factors include increased energy requirements and metabolic alterations. Cardiac cachexia is more commonly seen in dogs than in cats, and in dilated cardiomyopathy (DCM) or right-sided heart failure. The primary energy source for animals with acute or chronic disease is amino acids from muscle, thus causing a reduction in lean body mass. Cachexia is a slow, progressive process of the loss of lean body mass/muscle.
Careful examinations of obese animals should take place, as lean body mass reduction can occur, creating overcoat syndrome, and can be easily missed.
Any clinical nutrition of these animals includes management of any inappetence or anorexia if present, and referral back to the veterinary surgeon.
L-carnitine is critical for fatty acid metabolism and energy production, and cardiac myocytes depend on the oxidation of fatty acids for their energy. L-carnitine deficiencies and a causative link with DCM have been established.
L-carnitine deficiencies within the cardiac myocytes occur in 50% of dogs suffering with DCM. Some affected dogs with DCM do respond to L-carnitine supplementation. Carnitine supplementation of 50mg/kg to 100mg/kg bodyweight orally every eight hours has been recommended to dogs with DCM1, though most cardiac diets are already supplemented with L-carnitine.
The role of fatty acids in the diet of cardiac patients has been widely reported. Supplementation of the diet with EPA and DHA has shown to improve cachexia scores, but did not affect survival time; quality of life scores were improved, though. Animals suffering from cardiac cachexia do have an increased production of inflammatory cytokines. These cytokines are directly linked to causing anorexia, increasing energy requirements and increasing catabolism of the lean body mass1.
Supplementation of the diet with omega-3 fatty acids (EPA and DHA) does decrease the production and effects of cytokines. Recommended dosage of 40mg/kg bodyweight of EPA and 25mg/kg bodyweight of DHA for both dogs and cats with anorexia or cachexia have been noted1.
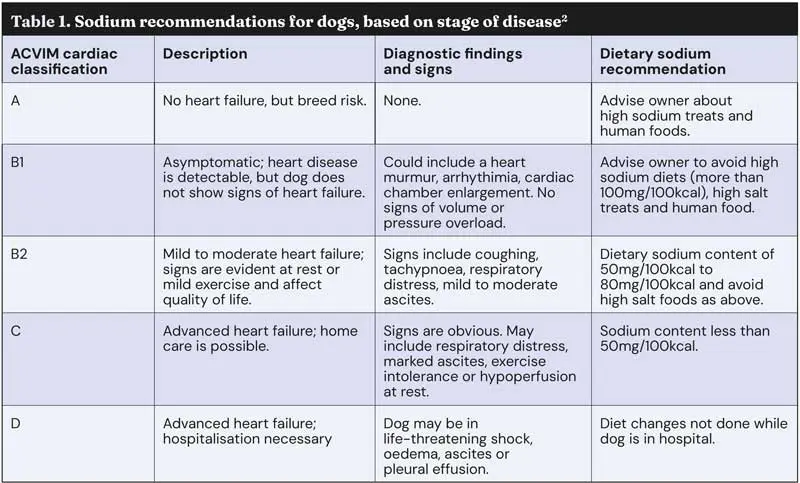
Medium-chain triglycerides (MCTs) have been shown to have a large positive effect on mitochondrial function in the cardiomyocytes. MCTs do not require carnitine-mediated transport to cross the mitochondrial membrane. They are, therefore, readily available as an energy source in the cardiomyocytes. MMVD has been classified by the American College of Veterinary Internal Medicine (ACVIM) into five stages (Figure 1). Diets supplemented with MCTs have been shown to slow the progression of MMVD in dogs currently in stage B2 into C.
Defined nutritional recommendations have been made for MMVD dogs based on the ACVIM classification (Table 1)2.
The level of carbohydrates in the diet has to support adequate calories for the specific life stage. As most cases will be in senior animals, the calorific value of the diet does need to reflect the body condition score.
It should also be remembered that these animals do tend to have a more sedentary lifestyle due to the cardiac disease, and the risk for weight gain or obesity is greater.
The recommended fibre levels in the diet are very much dependent on the individual. Fibre should be present, but not excessive in the diet. The presence of high-fibre levels in the diet does reduce the bioavailability of many pharmaceuticals, it should be noted on the medication’s information leaflet regarding administration and feeding intervals.
The nutrients of main concern in patients with heart failure include sodium, potassium and magnesium. Treats and snacks, which are often fed to dogs, do have a high salt content, as do cheese and processed meats, which are often used to administer medications. The restriction of sodium in the diet is useful in the mechanism to reduce fluid retention that accompanies many forms of heart disease.
Both sodium and water can be retained when the renin-angiotensin-aldosterone (RAA) cascade is stimulated, or when the patient’s blood pressure falls3. One of the current methods of treatment for fluid retention is the use of diuretics. The diuretics block sodium retention, but also promote urinary loss of magnesium and potassium. The prolonged use of diuretics can also lead to deficiencies of the water-soluble vitamins.
As a result of the cascade being stimulated, extracellular and vascular fluid volume increase, thus increasing preload. The plasma protein concentration therefore becomes more dilute, which in turn decreases plasma oncotic pressure. Water moves from the vascular to the interstitial compartment resulting in oedema, ascites and congestion. The use of angiotensin-converting enzyme (ACE) inhibitors has led to modification of the recommendation for sodium restriction, from senior diets and early cardiac disease diets. ACE inhibitors are designed to block the production of angiotensin II and its subsequent stimulation of the secretion of aldosterone. Both of these chemicals promote retention of water and sodium by the kidney. Thus, ACE inhibitors result in impaired sodium and water excretion.
Sodium intake needs to be limited in proportion to the severity of the disease (Table 1), in an attempt to avoid excesses. ACE inhibitors can also cause the retention of potassium; periodic serum levels should be monitored2.
Spironolactone has similar potassium sparing effects, along with being an aldosterone antagonist. CRF is often a concomitant disease of patients with cardiovascular disorders. Diets for these animals also need restricted phosphorous levels. Levels of potassium and magnesium should also optimally be controlled, as it supports the patient receiving diuretics and/or ACE inhibitor therapy. Magnesium levels can have a deleterious effect on a range of cardiovascular conditions, including hypertension, congestive heart failure, coronary artery disease and cardiac arrhythmias2.
Hypomagnesaemia can be induced through the use of digoxin and loop diuretics.
The B vitamin complexes are often supplemented into cardiac diets. At present there has been little investigation into the role of vitamin B deficiency as a cause of heart disease in dogs and cats. Polyuria and anorexia can both contribute to low vitamin B concentrations, and thus, higher B vitamin requirements are needed.
Taurine is an essential amino acid in cats, due to taurine being the only amino acid able to combine with cholesterol during bile salt synthesis, whereas in other species, another amino acid, glycine, can be substituted. Cats do have a limited ability to synthesis taurine from cysteine and methionine, but its use outstrips production. The mechanism of heart failure in cats and dogs with taurine deficiency is poorly understood.
Before 1987, supplementation of commercial foods with taurine was not commonplace and the number of cases of feline DCM was large.
Clinical studies have also shown that inadequate potassium intake may be sufficient to induce a significant taurine depletion and cardiovascular disease in cats. Most dogs presenting with DCM do not tend to have a concurrent taurine deficiency.
Although in some breeds where DCM is not a common disease, a taurine deficiency has been noted.
Dog breeds reported to be associated with taurine deficiency include the American cocker spaniel, golden retriever, Labrador, Newfoundland, Dalmatian and English bulldog1.
The overall protein level in the diet is reduced. This is due to the progression of renal disease, which is associated with cardiac disease. The protein levels are, therefore, restricted, but of a high biological value; typical values of 17% (dry matter basis; DMB) for dogs and 29% (DMB) for cats are often recommended.
Much debate surrounds grain-free diets and DCM in dogs. There is still no definitive evidence to support or refute the links between them, or the role of legume-based diets in the prevalence of DCM in predisposed breeds.
Some animals that have developed DCM while being on a specific diet have had their clinical signs either partially or completely resolved with a dietary change. Research is ongoing, and where grain-free, legume-rich test diets have been studied, they have caused reduced erythrocyte counts and hyperphosphataemia, findings also indicated in dogs with suspected DCM4,5.
Changes in taurine metabolism were indicated. This really highlights the importance of taking a very detailed nutritional history for all cardiac patients and giving good nutritional advice.
Nicola Lakeman works as the nutrition manager for IVC Evidensia. Nicola graduated from Hartpury College with an honours degree in equine science and subsequently qualified as a veterinary nurse in 2002. Nicola has written for many veterinary publications and textbooks, and is the editor of Aspinall’s Complete Textbook of Veterinary Nursing. Nicola is one of the consultant editors for The Veterinary Nurse. She has won the BVNA/Blue Cross award for animal welfare, the SQP Veterinary Nurse of the Year, the SQP Nutritional Advisor of the Year and, in 2024, the BSAVA Bruce Vivash Jones Award, which is presented annually by the BSAVA as the primary recognition for outstanding contributions to the advancement of small animal veterinary nursing. Nicola has recently gained her Master’s degree in advanced veterinary nursing from the University of Glasgow.