24 Feb 2026
Kathryn Patel BSc(Hons), BVetMed(Hons), CertAVP(G-SAS), CertVBM discusses how to support owners of pets with this chronic and progressive condition.
Kathryn Patel
Job Title
Image: Seventyfour / Adobe Stock
Osteoarthritis (OA) is a chronic, progressive, painful condition with a profound welfare impact, which commonly affects companion animals of all ages including rabbits, cats and dogs (Arzi et al, 2011; Lefort-Holguin et al, 2025; Meeson et al, 2019).
Consensus guidelines on management of chronic pain in humans emphasises the need for a person-centred multimodal strategy, focused on improving functional capacity and quality of life rather than solely eliminating pain (National Institute for Health and Care Excellence, 2021).
Increasingly, the veterinary profession is recognising the need to approach OA pain in pets similarly, and integrated mobility clinics such as VOA’s Vet-IMPACT are becoming the standard of care. Their success relies not just on clinical protocols, but also on effective engagement of pet caregivers.
This article suggests practical approaches for all members of the patient care team to employ to transform pet owners from passive recipients into proactive team members.
By acknowledging the owner as an expert on their pet’s day-to-day life and engaging in shared decision-making, the clinical team strengthens trust and supports mutual understanding of goals and limitations. Direct correlation exists between quality of communication during a consultation and client compliance, which has been a documented barrier to optimal care for at least 20 years (American Animal Hospital Association, 2003; Shaw and Coe, 2024; Singler, 2025).
To achieve collaborative care, the clinician must provide the client with all the necessary information about their pet’s condition and the available treatment options, and then work with the client to co-create a plan that is both medically sound and fits the values, preferences and circumstances of the caregiver.
Co-creation of treatment plans starts with achieving consistency in consultation structure between team members – especially when a multi-disciplinary team is involved.
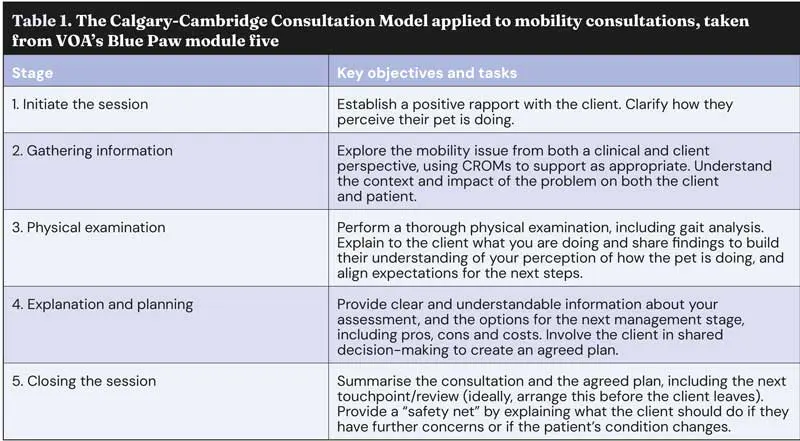
Many will be familiar with the Calgary-Cambridge consultation model (Table 1). This can be combined with key practical skills to improve client understanding and motivation to follow the agreed plan.
Active listening. Pay attention to verbal and non-verbal cues from the caregiver, and reflect what you understand to ensure comprehension.
Open-ended questions. Encourage caregivers to frame the consultation around their priorities based on their assessment of what’s important to the pet. Show empathy to build rapport and help them feel comfortable sharing their concerns.
Signposting. Help the client to navigate the consultation structure, so they know what to expect.
Chunk and check. Break down complex information into manageable chunks and check in with the caregiver that they understand before moving on.
Visual and written aids. Use diagrams, models, videos and handouts (physical or digital) to make information accessible to those with different learning styles and aid retention of information after the consultation.
Consultations should provide ample time and a supportive environment, allowing owners to voice their observations and concerns. In-depth discussions enhance understanding of each pet’s unique situation and build owner trust. At assessment, incorporating home-based questionnaires and explicitly valuing the owner’s perspective in clinical decision-making creates a collaborative partnership.
A cornerstone of owner engagement is the use of clinical metrology instruments (CMIs), also known as client-reported outcome measures (CROM). These validated, species-specific questionnaires (for example, Liverpool Osteoarthritis in Dogs; Helsinki Chronic Pain Index; Feline Musculoskeletal Pain Index) convert owner observations into structured scores, providing semi-objective data to guide clinical decisions.
For clarity, “validated” is a term defined as the questionnaire being able to measure what it intends to measure (Ranganathan et al, 2024); for example, do the questions within the questionnaire itself enable responders to differentiate between different levels of their pet’s lameness?
For some CMIs, such as Liverpool Osteoarthritis in Dogs (LOAD), the validation goes a step further, with force-platform analysis having been performed at the time of questionnaire validation. In LOAD, this assessment identified a statistically significant weak correlation between LOAD scores and peak-vertical force symmetry index. This means that LOAD can be used as a simple instrument for the measurement of canine OA: convenient to use, validated, and having some correlation with force-platform data (Walton et al, 2013).
CMIs are particularly valuable in chronic, fluctuating diseases such as OA; they capture pets’ behaviours at home, measure pain and functional change, and give owners a meaningful, ongoing task. New tools, such as the GenPup-M CMI (accessible in the UK as the DogMA App), allow proactive, app-based monitoring of mobility, with automated reminders to promote regular completion.
Engagement is achieved when owners see tangible evidence of the efficacy of interventions in their pet’s journey. Demonstrating improvement, celebrating milestones, and providing timely feedback and solutions ensures owners understand why they are doing something and can see that it is working.
Both objective and subjective monitoring are required to turn a series of consultations into a long-term care pathway.
Subjective monitoring is the client’s qualitative perception and experience of their pet’s condition, such as “she wants to play again”, “his appetite is back to normal”, or rating their pet’s pain on a 1-10 scale. It is often more compelling to caregivers than objective data and feels more tangible and relatable. It is also likely to be the earliest warning the clinical team get where barriers to compliance exist, such as, “he doesn’t like the new tablets”. Early recognition of barriers allows support of caregivers before non-compliance occurs.
Objective monitoring is quantitative, measurable and unbiased data, usually collected by the clinical team, such as body condition score, range of motion measured in degrees, gait analysis or validated clinical metrology instrument scores. It is important to validate treatment efficacy – especially where improvements are slow, which could lead to abandonment of effective interventions, and also to enable agile adjustments in the case of deterioration or non-response to treatment. It can also be used to challenge subjective assumptions that may be based on placebo effect, misinterpretation or masking of clinical signs, or projection of the caregiver’s emotional state.
When faced with a subjective impression that seems wrong, the professional’s role is crucial:
Never dismiss. Always validate the observation (“That’s really helpful information”). Dismissing their view will instantly break trust.
Ask for specifics. Move from the general to the specific. Instead of accepting, “he’s better”, ask, “what is he doing now that he wasn’t before?”. This can help separate vague feelings from concrete facts.
Educate gently. Explain the clinical reasoning: “I understand completely why you’d think moving around more is a good sign. However, in a patient with painful joints, being unable to settle and get quality rest could be a sign of discomfort.”
Anchor with objective data. Use objective findings to guide the conversation: “I hear that you’re not seeing much of a limp at home, which is great. When I watch her walk, I can see reduced weight bearing on the bad leg. This tells us there’s still some discomfort, which is why it’s so important we continue to use anti-inflammatory treatment.”
A co-created treatment plan requires shared goals and accountability. Combine subjective and objective targets; for example, set a subjective goal to be able to jump on the sofa again, and an objective goal to increase muscle condition score by one point.
All members of the care team – caregiver, vet, veterinary nurse, and physiotherapist, or any other paraprofessionals – should be aware of these goals, so they can contribute to them. Keeping a standardised record (or diary) of each visit captures progress toward goals, objective data points, treatments/interventions and any concerns to keep things on track.
Where barriers to compliance exist, tackling these early helps improve overall success. Owners may have economic or practical constraints; it is important to prioritise manageable interventions and set realistic goals. Encouraging caregivers to lead consultation and treatment planning ensures communication and care can be contextualised.
Remember, it is important to contextualise to caregivers as well as pets and budgets; many of the adult population has low health literacy, which is the degree to which an individual has the capacity to obtain, process and understand basic health information, and make appropriate health decisions (Novotny and Wayner, 2019). This can have an impact on their ability to understand and follow veterinary recommendations, so it is crucial to ensure that communication is understood.
In summary, pet caregivers are best positioned to notice subtle changes in their pet, and implement home modifications.
Musculoskeletal disease accounts for around eight per cent of presentations to GP veterinary practices in the UK (O’Neill et al, 2021), so investment in owner education and engagement not only stands to improve clinical outcomes and welfare, but also client and staff satisfaction, and practice reputation, leading to better returns for the practice as a business.
Regularly review your clinic’s owner engagement strategies. Small, consistent improvements will pay dividends in compliance, outcomes, and team morale.
A young feline patient with underlying patellar and dental syndrome sustained bilateral patellar fractures before two years of age, managed with a combination of surgical and conservative approaches. After almost a year without medication, the owner, acting as an essential member of the mobility care team, observed subtle changes in her pet’s mobility, including climbing rather than jumping on to the bed and altered pelvic limb gait.
These observations led to further veterinary assessment, which in addition to confirming ongoing secondary changes attributable to the historic patellar injuries, revealed new changes in the thoracolumbar vertebrae.
In direct response to the owner’s vigilant reporting and involvement, the treatment plan was updated to include analgesic and anti-inflammatory medication, initiation of physiotherapy, and neurology referral.
Osteoarthritis is not just a joint problem; it affects mobility, comfort, behaviour, longevity and overall quality of life. The VOACON 2026 programme brings together new expert speakers alongside familiar favourites, delivering practical, evidence-based insights you can apply immediately to elevate your OA care. Visit this site to book.
Kathryn Patel is an advanced practitioner in small animal surgery with extensive clinical experience. Passionate about modernising the approach to osteoarthritis (OA) and chronic pain, Kathryn is dedicated to removing barriers to earlier, better care for patients. Her work focuses on advancing practical solutions that improve outcomes and support veterinary professionals in tackling OA more proactively.
