Chronic canine gastrointestinal disease: diagnosis and treatment
Christina Maunder discusses, in the second of a two-part article, methods for diagnosing, treating and managing cases of chronic gastrointestinal disease
Christina Maunder
Job Title
Figure 1. A SNAP ELISA test kit.
Chronic vomiting or diarrhoea will have, by definition, persisted for more than two weeks and is not self limiting. A logical approach is necessary to achieve a diagnosis and instigate appropriate treatment.
Diagnostic approach
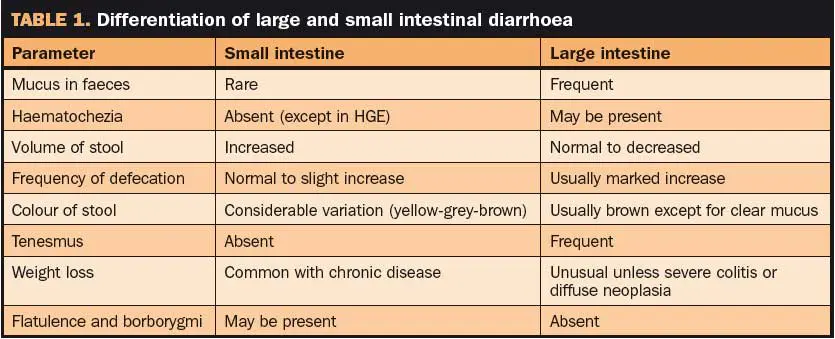
The signalment may be useful in aiding you to prioritise the differential diagnosis list (Table 1).
– Age: as an example, idiopathic inflammatory bowel disease (IBD) is unlikely in dogs younger than one year of age, while infections or dietary sensitivity are more common.
– Breed: German shepherd dogs, for example, are predisposed to exocrine pancreatic insufficiency (EPI), antibiotic responsive diarrhoea and IBD.
History. As with all medical investigations, history is essential. Ensuring correct identification of the primary problem may help you localise gastrointestinal (GI) disease. Distinguishing regurgitation from vomiting is important, as it helps to rule out oesophageal disease. Likewise, differentiating whether small intestinal or large intestinal signs predominate with diarrhoea can alter the diagnostic approach (Table 1). A dietary history and details of any medication, vaccination and worming status may also prove helpful.
Physical examination. The gastrointestinal tract is relatively hard to assess by physical examination. Oral examination may demonstrate uraemic ulcers or a linear foreign body. Abdominal palpation may reveal pain or the presence of a surgical disease (intussusception, foreign body or mass). Rectal examination may reveal rectal, anal or anal sac lesions, diarrhoea, melaena or constipation.
Routine blood analysis. Haematology and biochemistry should be performed in order to rule out extra-gastrointestinal causes of vomiting and diarrhoea. In many chronic cases of GI disease, no abnormalities will be detected on a routine profile. Occasionally, dehydration may cause mild changes to be observed (haemoconcentration, elevated total protein measurements or pre-renal azotaemia).
A mild non-regenerative anaemia is also a non-specific finding with chronic inflammation or disease. Certain GI diseases can cause more significant changes to a routine blood profile: panhypoproteinaemia may result from a protein-losing enteropathy; a disproportionately elevated urea compared to creatinine can be suggestive of gastrointestinal haemorrhage; and microcytic hypochromic anaemia is also consistent with chronic gastrointestinal haemorrhage.
ACTH stimulation test. This is used for hypoadrenocorticism, particularly in patients where intermittent gastrointestinal signs are indicated.
Bile acid stimulation test. This is indicated if there is any doubt as to interpretation of elevated hepatic enzymes or hepatic function from a routine biochemistry profile.
Urinalysis. This may be necessary to rule out proteinuria and demonstrate an appropriate specific gravity in a patient with azotaemia due to dehydration.
Faecal analysis. Parasitology (to detect protozoa and roundworms) is mandatory in all chronic cases of diarrhoea before further investigation is undertaken. Giardia infection may be harder to detect, and three consecutive zinc flotation tests are recommended. Alternatively, a SNAP ELISA test exists (Idexx; Figure 1) for in-house use. Microbiology in cases of chronic diarrhoea is more difficult to interpret.
Positive cultures, particularly Campylobacter species, can be found in healthy dogs, and so isolation of bacteria does not necessarily indicate this is the cause. The potential for C jejuni and Salmonella species to be zoonotic means owners must be informed, but the decision to treat may be based on the environment at home (for instance, in-contact children or immunosuppressed individuals), presence of concurrent disease (co-infection may result in more severe disease) and clinical signs (haemorrhagic enterocolitis and possible septicaemia).
Gastrointestinal-specific blood tests.
– Canine pancreatic lipase is indicated in cases of vomiting, abdominal pain and anorexia. Pancreatitis may also be a cause of gastrointestinal haemorrhage (the duodenum and colon are most affected due to their anatomical proximity to the pancreas).
– Trypsin-like immunoreactivity should be measured in patients with chronic diarrhoea to rule out exocrine pancreatic insufficiency.
– Serum folate and cobalamin can be measured to give an indication of the presence of infiltrative disease within the small intestine. These water-soluble vitamins are absorbed from the small intestine, and severe or prolonged infiltrative disease may result in malabsorption and reduced serum levels. Folate is absorbed from the proximal small intestine (jejunum) and cobalamin (vitamin B12) from the more distal segment (ileum). In theory, a selective reduction in one or the other may help localise the site of disease further. The pattern of increased folate and decreased cobalamin described for bacterial overgrowth is not reliable for diagnosis of this condition.
Radiography. Plain films are indicated to rule out extra-intestinal disease and obstructive GI disease. Contrast studies are time consuming and rarely add significant information in chronic cases of vomiting or diarrhoea.
Abdominal ultrasound. This is extremely useful for examination of the gastrointestinal tract and other abdominal organs, in particular the pancreas, liver and abdominal lymph nodes. Obstructive GI disease may be identified on ultrasound. More specifically, ultrasound allows the visualisation of gastric and intestinal wall thickness, layering and echogenicity. Normal layering is more likely to be disrupted by an infiltrative process, such as neoplasia, than with IBD. Increased thickness of the gastric or intestinal walls may be seen with IBD if layering is retained, but it can also result from oedema. Gastric ulceration, pyloric hypertrophy and focal mass lesions may all be detected.
Intestinal biopsy. In many cases of chronic disease, intestinal biopsy is necessary to establish a diagnosis. Two main methods are available for collection of biopsies: endoscopic (mucosal samples) and surgical (full thickness).
Endoscopic biopsy is a safer procedure, as the general anaesthetic is the biggest risk to the patient. Ideally, this would be the first choice, unless the investigation to this point had localised the disease process to the jejunum and, therefore, out of endoscopic reach, or if endoscopy is unavailable. Surgical biopsy allows full thickness intestinal samples and, therefore, can be more helpful for some histopathological diagnoses, when it is critical to determine the degree of involvement of the submucosa. Wound dehiscence is a serious complication of the procedure and rates of up to 12 per cent have been reported (Shales et al, 2005). Patients with severe hypoproteinaemia might also be excluded due to poor wound healing.
Treatment and management of IBD
By definition, IBD patients have inflammatory changes on histopathology samples. However, this is a pathological finding and not an aetiological diagnosis. Idiopathic IBD is a diagnosis of exclusion and inflammatory changes due to dietary sensitivity, and chronic infection (parasite, bacterial) must be eliminated. Consequently, management of these cases often involves stepped therapeutic trials.
Mild cases may well respond to dietary manipulation and antibacterial therapy. More severe cases will need immunosuppressive drugs, and delaying the introduction of this medication may not be possible. If a full diagnostic investigation is not possible for financial, personal or technical reasons then an empirical approach to these cases may be undertaken.
Anthelmintic/antiparasiticide therapy. Fenbendazole (Panacur) 50mg/kg q24hrs per os for three to five days is recommended to eliminate infections that may be hard to detect, in particular Giardia species.
Dietary sensitivity. This diagnosis encompasses food intolerance (a non-immunologic diagnosis) and food allergy (an immunologic event).
– Food intolerances can be unpredictable and may have no changes on histopathology, making them hard to diagnose.
– Food allergies may cause type-one (anaphylactic) reactions or delayed type-four hypersensitivity reactions. The principle is a repeatable adverse reaction to a specific food or additive. Beef, dairy products and gluten are commonly implicated in dogs.
– Feeding a single, novel source of protein and carbohydrate should result in elimination of the clinical signs. Usually, a three-to-four week trial is sufficient time to assess the response. Confirmation of the diagnosis can be made by reintroduction of the normal diet. This challenge should cause a relapse in clinical signs. Compliance can be an issue with exclusion diets, as nothing else must be fed during the trial period. Identifying a novel source of protein and carbohydrate can also be difficult. Hydrolysed diets (Purina HA, Hill’s z/d) offer an alternative if no commercial novel source can be found.
– Restoration of an exclusion diet after the diet challenge also allows for provocation testing. Single food stuffs can be reintroduced in turn to try to determine which protein or carbohydrate a dog reacts to and that induces clinical signs. This may enable a cheaper or more accessible maintenance diet to be fed long term – provided the relevant foodstuffs are avoided.
Antibacterial therapy. Trial therapy is justified on the grounds of eliminating any undiagnosed enteropathogens and modulating the intestinal flora that may reduce the degree of inflammation present (breakdown of immunotolerance to bacterial antigens is thought to be involved in the pathogenesis). Many of the commonly used drugs also appear to have an immunomodulatory role. Metronidazole (10mg/ kg per os bid) is commonly used. Oxytetracycline (10mg/ kg per os tid) is an alternative. A three-to-four week trial is again recommended if the severity of signs allow this.
Immunosuppressive therapy. Ideally, this should only be used if histopathology has confirmed the presence of inflammatory changes and other treatment modalities have failed. These drugs are the most important treatment modality in severe idiopathic IBD. Empirical therapy should only be used with owner consent and warning of the risks, the potential to exacerbate signs and inability to then pursue further investigation in the short term. Prednisolone 1.0mg/kg bid is normally recommended for three to four weeks, and then the dose tapered over the following weeks – months if possible. If the side effects of the prednisolone are excessive or the clinical signs are not controlled, adjunctive therapy may be needed. Azathioprine has been used (2mg/kg per os sid), but this may have a delayed onset of activity of up to two weeks. Myelosuppression is rare, but can occur quickly (one to two weeks), so regular monitoring of haematology is necessary. Ciclosporin (5mg/kg per os sid) was used in a study of steroid-resistant dogs (Allenspach et al, 2006) and may show promise, but is expensive. Budesonide is an alternative glucocorticoid with reduced systemic side effects (due to high first-pass hepatic metabolism), however, there is limited information available in dogs, the optimal dose has yet to be determined and it is more expensive than prednisolone.
Overall, the prognosis for patients with idiopathic IBD can be variable. In some cases, an initial good response can result, but a later relapse that is refractory to further treatment then occurs. A retrospective study (Craven et al, 2004) quoted 26 per cent of cases had full remission, 50 per cent had intermittent signs, four per cent were completely uncontrolled and 13 per cent were euthanised due to lack of response. A negative outcome has been associated with severe disease (histologically), hypoalbuminaemia, concurrent pancreatic disease and hypocobalaminaemia.
Adjunctive therapies. Other therapies may help reduce the clinical signs experienced, particularly in the early stage of a therapeutic trial. They may be insufficient to control the signs on their own, but they have a steroid-sparing effect and a multi-modal approach may give a better clinical outcome.
5-aminosalicylic acid (5-ASA) derivatives. Dogs with signs limited to the large intestine may be prescribed sulfasalazine (Salazopyrin) 15mg/ kg to 30mg/kg per os bid or tid. Colonic bacteria cleave the diazo bond to release the 5-ASA (NSAID) from the sulphonamide carrier. The 5-ASA can then act locally at high concentrations. The major side effect is kerato-conjunctivitis sicca.
Probiotics and prebiotics. Modulation of the enteric flora could have benefits in reducing the antigenic trigger for IBD. Mouse models and placebo-controlled trials in man have shown promise, but further studies are needed in dogs.
Soluble fibre. Psyllium or beet pulp, etc can be useful in cases of large intestinal disease. The fermentable fibre is metabolised by colonic bacteria to provide short-chain fatty acids (a source of energy). This promotes colonic epithelial health. Psyllium has a great water holding capacity and forms a gel in water, thereby improving faecal consistency.
Cobalamin (vitamin B12). Hypocobalaminaemia should be addressed, as this can cause systemic metabolic consequences. Parenteral supplementation should be administered until serum levels are restored (0.25mg to 1.0mg SC every seven days for four weeks, then every 28 days for three months, or as necessary).
Helicobacter species
The causal relationship between Helicobacter pylori and gastric disease in man has now been firmly established. The presence of gastric Helicobacter – like organisms in dogs – has been known for years, but their significance remains controversial. Finding Helicobacter in a dog with chronic vomiting justifies the use of triple therapy only after all other causes of vomiting have been eliminated. Therapy typically comprises amoxicillin 15mg/ kg per os bid; metronidazole 10mg/kg per os bid and bismuth subsalicylate 65mg/kg to 524mg/ kg per os bid) or dual therapy (amoxicillin 15mg/kg per os BID and clarithromycin 7.5mg/kg per os bid for 14 days. Some dogs will significantly improve with treatment, supportive of the significance of Helicobacter, while others will remain unchanged.
Antibiotic-responsive diarrhoea
Idiopathic antibiotic-responsive diarrhoea (ARD), which was previously known as small intestinal bacterial overgrowth (SIBO), is most commonly reported in young German shepherds, but has also been seen in other breeds. Secondary SIBO can occur with partial obstructions, abnormal anatomy, mucosal disease, EPI and motility disorders.
No changes are usually seen on histology in these cases. Most cases are treated with metronidazole (10mg/kg per os bid) or oxytetracycline (10mg/kg per os tid) for four to six weeks. Some dogs will require longterm therapy to control the signs, while others can be maintained on decreased frequency of dosing, and some will resolve. Secondary cases will improve with antibiotics, but the underlying cause must be addressed.
Irritable bowel syndrome
This term has been applied to dogs with chronic idiopathic large bowel signs that usually exhibit mucoid diarrhoea and tenesmus. No underlying cause has been identified, but cases may respond to the feeding of a highly digestible diet with soluble fibre added.
Lymphangiectasia
This is characterised by marked dilatation and dysfunction of intestinal lymphatics, which may be primary or secondary to infiltrative intestinal disease. The leakage of protein-rich lymph fluid into the gastrointestinal lumen results in hypoalbuminaemia. Diagnosis is confirmed on intestinal biopsy. Dietary management (marked fat-restricted, highly digestible, calorie-dense diets) and prednisolone (1.0mg/ kg per os bid) are the main therapies. Supplementation with fat-soluble vitamins is advised.
This article appeared in Vet Times (20 September 2010), Volume 40, Issue 37, Pages 6-8
References
Allenspach K, Rufenacht S, Sauter S, Grone A, Steffan J, Strehlau G, Gaschen F (2006). Pharmacokinetics and clinical efficacy of cyclosporine treatment of dogs with steroid refractory inflammatory bowel disease, Journal Veterinary Internal Medicine20(2): 239-244.
Allenspach K (2010). Diseases of the large Intestine. In Textbook of Veterinary Medicine 7th Edn. Ettinger S J and Feldman E C (eds). Saunders, Elsevier, St Louis, Missouri.
Craven M, Simpson J W, Ridyard A E, Chandler M L (2004). Canine inflammatory bowel disease: analysis of diagnosis and outcome in 80 cases (1995-2002), Journal of Small Animal Practice45(7): 336-342.
German A J (2009). Inflammatory Bowel Disease. In Kirk’s Current Veterinary Therapy XIV ed. Bonagura J D and Twedt D C. Saunders, Elsevier, St Louis, Missouri.
Hall E J (2009). Canine diarrhoea: a rational approach to diagnostic and therapeutic dilemmas, In Practice 31: 8-16.
Hall E J, German A J (2010). Diseases of the small intestine. In Textbook of Veterinary Medicine 7th Edn. Ettinger S J and Feldman E C (eds). Saunders, Elsevier, St Louis, Missouri.
Ramsey I (2008). BSAVA Small Animal Formulary 6th Edn. BSAVA, Cheltenham, UK.
Shales C J, Warren J, Anderson D M, Baines S J, White R A S (2005). Complications following full-thickness small intestinal biopsy in 66 dogs: a retrospective study (2005), Journal of Small Animal Practice46(7): 317-321.
Simpson K W (2010), Diseases of the stomach. In Textbook of Veterinary Medicine 7th Edn. Ettinger S J and Feldman E C (eds). Saunders, Elsevier, St Loius, Missouri.
Simpson K W, Neiger R, DeNovo R, Sherding R (2000). The Relationship of Helicobacter spp infection to gastric disease in dogs and cats – ACVIM Consensus Statement, Journal of Veterinary Internal Medicine 14: 223-227.