19 May 2026
Karina Fresneda DVM, DipIACVP explains why stretching and squeezing matter for detecting Demodex and Sarcoptes.
Karina Fresneda
Job Title
Image: kobkik / Adobe Stock
In an era dominated by molecular diagnostics, advanced imaging and the rise of AI, it’s easy to overlook the humble skin scrape.
Yet this simple procedure remains the diagnostic cornerstone for some of the most common parasitic skin diseases in veterinary practice. When performed correctly, it is rapid, inexpensive and immediately informative. However, poor technique or incorrect interpretation risks false-negative results that can delay diagnosis.
The diagnostic value of skin scrapes depends on how and where the sample is collected. Studies comparing deep skin scrapings with hair plucks, tape preparations and other sampling methods for demodicosis, and evaluations of conventional skin scrapings for sarcoptic mange, consistently show that suboptimal sampling technique is a major contributor to diagnostic failure. Understanding the biological behaviour of different mites – and adapting technique accordingly – is therefore essential.
This article focuses on the practical “art” of skin scraping, why this is important for detecting Demodex mites, and why even with excellent technique, skin scrapes may still fail to identify Sarcoptes scabiei.
Before considering skin scrape technique, it is important to understand how Demodex and Sarcoptes differ in their biology and behaviour. These differences largely explain why skin scraping can be highly rewarding in one disease and frustratingly unrewarding in the other.
Demodicosis is a common parasitic skin disease in dogs. Reported prevalence varies widely, ranging from approximately 0.4% to 23% in epidemiological studies, depending on population and diagnostic criteria1.
Three Demodex species are recognised as normal commensals of canine skin: Demodex canis, Demodex cornei and Demodex injai. All inhabit hair follicles and/or sebaceous glands, but when mites multiply in excessive numbers clinical disease may be seen. D canis is most commonly associated with generalised demodicosis, with D injai also implicated in some cases.
Demodicosis is commonly classified according to age of onset and extent of disease. Localised disease typically occurs in dogs below one year of age and often resolves spontaneously. Generalised demodicosis usually presents before 18 months of age, whereas adult-onset disease (after 1.5 years) is more often associated with underlying immunosuppression or concurrent disease.
The pathophysiology of demodicosis is not fully understood. Current evidence suggests that a temporary or inherited defect in cell-mediated immunity, particularly involving T-cell function, plays an important role in juvenile-onset disease2. In adult dogs, immunosuppressive conditions are frequently implicated, although other, as yet unidentified, factors may also contribute. It is also important to bear in mind that Demodex mites are part of the normal cutaneous microfauna, meaning that interpretation of diagnostic findings must always be made in the context of clinical signs.
Unlike Demodex, Sarcoptes scabiei var canis is a true pathogen with no commensal phase. These highly contagious mites are transmitted by direct contact with infected dogs or, less commonly, through contact with fox carcases or contaminated environments. The disease is zoonotic, though human lesions are typically self-limiting once the canine source is treated.
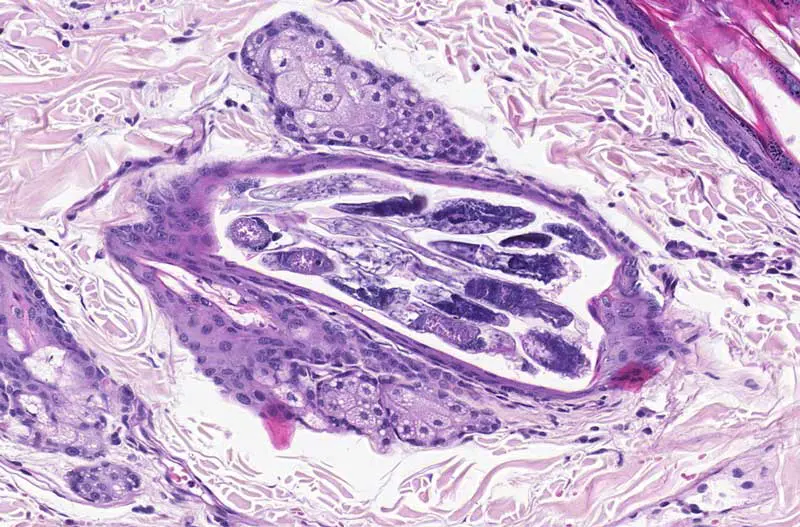
The life cycle and pathogenesis of Sarcoptes help explain why it can be so diagnostically challenging. Males and females mate on the skin surface, after which the female burrows into the upper layers of the epidermis, creating winding tunnels as she feeds on tissue fluid and cellular debris. Within these tunnels, eggs are deposited over a period of several months. The complete life cycle from egg to adult takes two to three weeks3.
Clinical signs are dominated by intense pruritus, largely attributable to a hypersensitivity reaction to mite antigens rather than to mite burden per se. This explains why even small numbers of mites can trigger severe clinical disease, and conversely, why finding mites on skin scrapes can be extraordinarily difficult. The most commonly affected sites include the ear pinnae, elbows, hocks and ventral abdomen. The pinnal-pedal reflex – a scratch response elicited by rubbing the ear margin – is positive in approximately 90% of cases and remains one of the most useful clinical diagnostic indicators3.
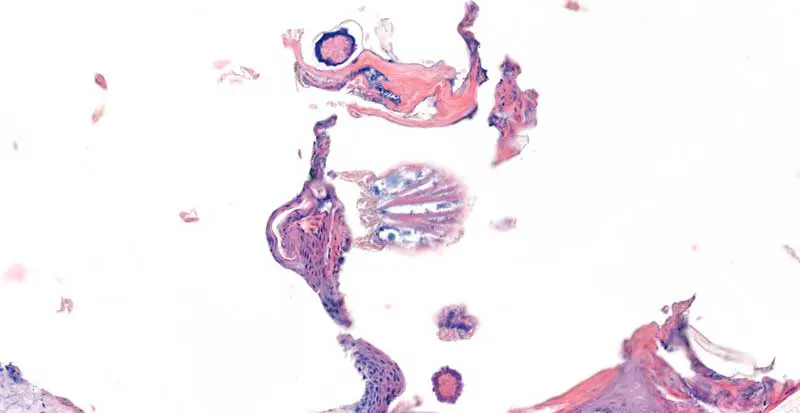
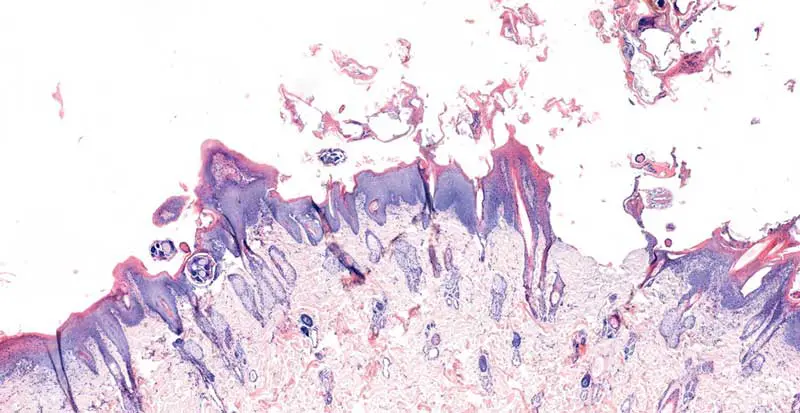
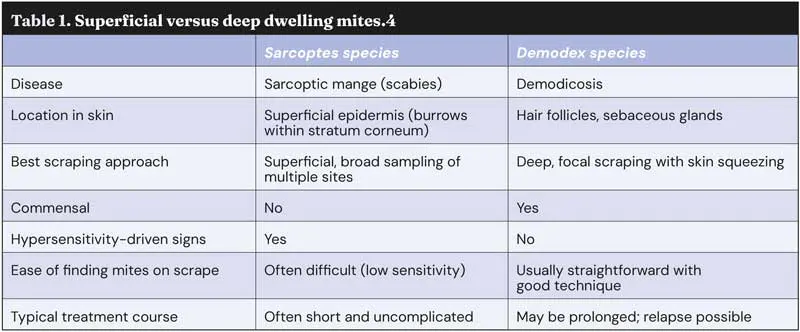
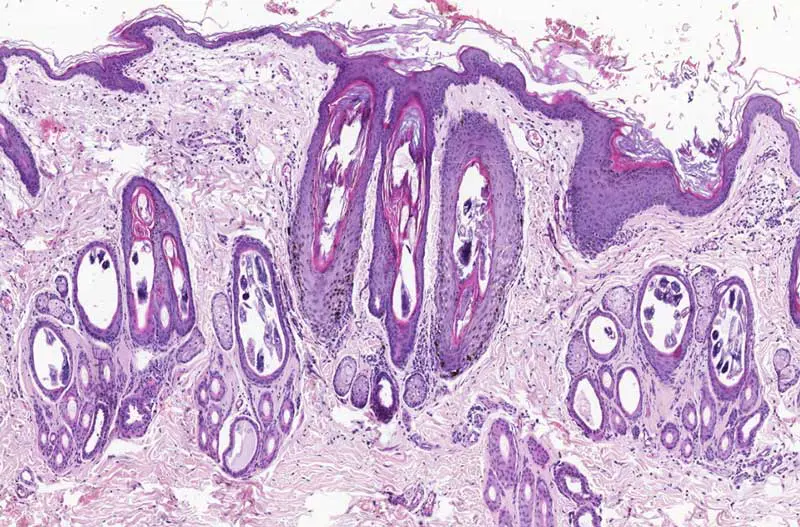
Table 1 summarises the fundamental differences between these two parasitic diseases and their implications for diagnosis and management. The location of each mite within the skin is perhaps the most important factor determining diagnostic approach. Demodex inhabits hair follicles and rarely sebaceous glands deep within the dermis. These structures run perpendicular to the skin surface, creating anatomical “silos” that protect mites from superficial sampling. Sarcoptes, by contrast, burrows within the epidermis itself, creating horizontal tunnels just beneath the stratum corneum. However, these tunnels are often covered by crusts and scales, and the female mite spends much of her time within the tunnel rather than on the surface.
The commensal status of Demodex has important interpretive implications. Finding one or two mites may simply reflect normal colonisation, whereas finding multiple mites – or mites in association with appropriate clinical signs – indicates pathological overgrowth. For Sarcoptes, any mite identified is diagnostically significant, though their scarcity means that negative scrapes are common even in confirmed cases.
The hypersensitivity component of sarcoptic mange means that clinical signs can be markedly disproportionate to mite numbers. A type IV hypersensitivity reaction typically develops around two to five weeks after initial infestation, resulting in intense pruritus that persists even when mite burdens are low. Demodicosis, in contrast, is largely a consequence of mite burden rather than a hypersensitivity reaction, meaning that clinical signs generally correlate with mite numbers.
In terms of treatment, the two conditions also differ. Sarcoptes is usually readily treated by modern acaricides, whereas demodicosis – particularly generalised forms – often requires a prolonged treatment course and may relapse if underlying predisposing factors are not addressed.
Deep skin scrapings remain the diagnostic gold standard for demodicosis. With good technique, reported sensitivities are usually higher than other methods, although tape squeeze preparations can sometimes be useful2,4. With skin scrapes, the key to success lies in understanding the mite’s location and squeezing the skin to physically bring mites from the depths of hair follicles to the scraped surface.
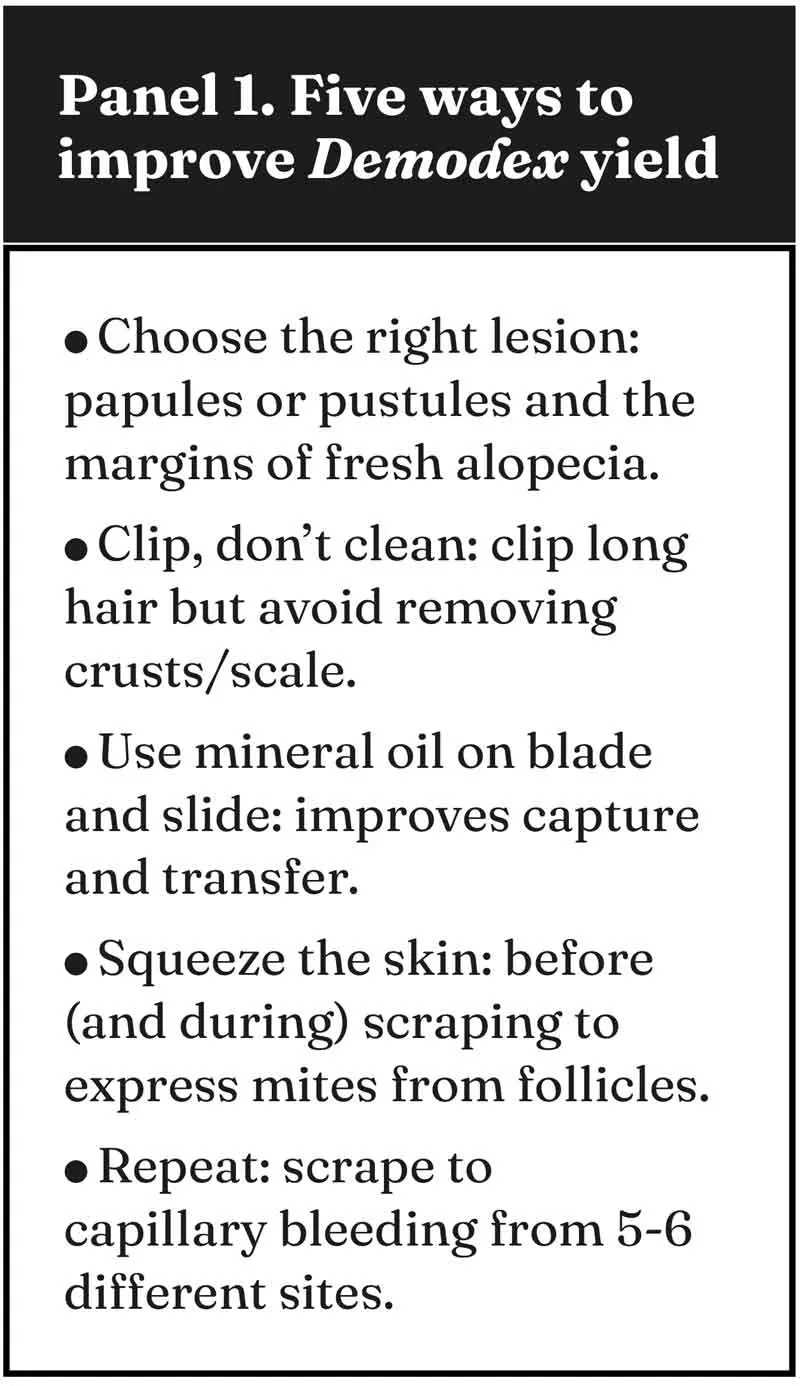
Site selection. Diagnostic yield is highest when sampling from active primary lesions. Follicular papules and pustules are ideal targets, as these represent sites of active mite proliferation and follicular inflammation. Areas immediately adjacent to papules, areas of crusting or obvious hair loss also tend to be productive.
In medium or long-haired breeds, clipping an area of skin before scraping, removes physical obstruction and allows better visualisation of the skin surface and any surface changes that might guide ideal sampling locations. Where crusting or scaling is present, avoid displacing this material during clipping, as it should be included in the sample.
Equipment and preparation. The equipment required is minimal: a number 10 scalpel blade, mineral oil, glass slides and coverslips. Place a drop of mineral oil on the blade before scraping – this aids adherence of scraped material to the blade during collection.
Squeezing and stretching. Before, and sometimes during scraping, firmly squeeze or pinch the skin between thumb and forefinger. Squeezing mechanically expresses Demodex mites from the depths of hair follicles toward the skin surface, dramatically increasing the number of mites available for collection and increasing the likelihood of an accurate diagnosis.
Stretching the skin taut makes skin scrapes easier to perform, but also serves an additional function. Hair follicles naturally lie at an angle to the skin surface. Stretching straightens these follicles, reducing the tortuous path that would otherwise shield mites. This is particularly important in areas where skin is mobile or naturally folded.
Depth and technique. Scrape firmly in the direction of hair growth until capillary bleeding occurs. This confirms that sufficient depth has been achieved to reach the hair follicles. The scraped area should be approximately 1cm², and multiple sites should be sampled. Five to six scrapes from different locations are usually recommended to maximise sensitivity, particularly when clinical suspicion is high, but initial scrapes are negative.
Transfer the collected material to a glass slide with a drop of mineral oil, apply a coverslip and examine under low magnification (x4 or x10 objective). Demodex mites are elongated and cigar-shaped, making them readily recognisable. Scan the entire sample systematically, as mites may be unevenly distributed. Examine samples promptly where possible as mite morphology may deteriorate over time, potentially affecting identification.
The diagnostic threshold is relatively straightforward: according to World Association for Veterinary Dermatology consensus guidelines, finding more than one Demodex mite on any given test is an indication of clinically relevant demodicosis.
All life stages may be observed, including adults, nymphs, larvae and eggs. The presence of numerous immature forms suggests active reproduction and further supports a diagnosis of demodicosis.
While good technique can improve diagnostic yield for demodicosis, the same cannot always be said for sarcoptic mange. Skin scraping has a low sensitivity for Sarcoptes, and negative results should never be used in isolation to rule out disease.
Reported sensitivities can be as low as 20%3, reflecting the typically low mite burden and the tendency for mites to remain within burrows rather than on the skin surface. In contrast to demodicosis, where repeated deep scrapes from appropriate sites usually yield mites when disease is present, repeated negative scrapes are common even in confirmed cases of scabies. As a result, any Sarcoptes mite that is identified on skin scraping is diagnostically significant.
When skin scrapings are inconclusive or impractical, additional diagnostic options should be considered, guided by the suspected underlying disease and the clinical context.
Sarcoptes serology. Serological testing for Sarcoptes-specific antibodies can be a useful adjunct, particularly in cases where skin scrapings are repeatedly negative. Antibodies typically become detectable four to eight weeks post-infection, reflecting the time required for seroconversion. Serology has high diagnostic reliability, with reported sensitivity of up to 95%5. Where a result is borderline, serology should be repeated after two weeks.
Results should always be interpreted alongside clinical signs and it is important to bear in mind that young animals and dogs receiving corticosteroids may have higher false-negative rates.
Histopathology. Biopsy is not a first-line test for most suspected mite infestations, but it has a role when clinical suspicion remains high despite repeated negative scrapes or when lesions are in sites that are difficult to sample effectively (for example, paws, periocular skin or severely thickened or crusted areas). For demodicosis, biopsy can also help confirm disease in chronic, thickened lesions.
For sarcoptic mange, biopsy has relatively low sensitivity because mites are few and may not be sampled.
However, histopathology may be most useful when the differential diagnosis list is broad or atypical features warrant ruling out other diseases.
Skin scraping remains one of the most useful point-of-care tests in small animal dermatology, but it is only as good as the technique behind it. For demodicosis, understanding the follicular location of Demodex mites can turn a low-yield scrape into a definitive diagnosis within minutes. For sarcoptic mange, the challenge is different: clinical signs may be striking despite very low mite numbers, so negative scrapes are common and should never be used to rule out disease. Ultimately, matching sampling method to mite biology reduces false negatives, speeds appropriate treatment, and improves outcomes for patients.
Karina Fresneda graduated from the National University of the Centre of Buenos Aires Province in Argentina in 2000, and after two years of training, she became a specialist in anatomo-histopathological veterinary diagnosis. She has been teaching in infectious diseases at the same university for 15 years. At the same time, Karina was gaining experience in her clinic and laboratory, as a clinician and working in clinical pathology, cytology and histopathology. She took a three-year residency in anatomic veterinary pathology at the University of California, Davis, where she received intensive training in this field. Karina also enjoys teaching different courses on clinical pathology, cytology and histopathology.