5 May 2026
Andrew Kent BVSc, DipECVIM-CA, MRCVS discusses presentation, diagnosis and treatment of this abnormality, more commonly seen in bitches.
Andrew Kent
Job Title
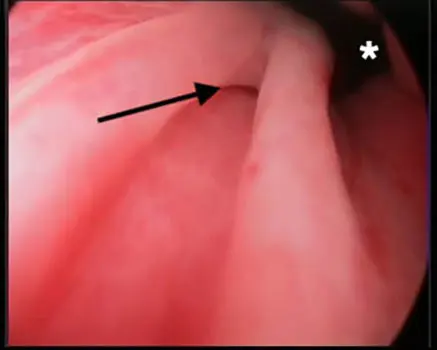
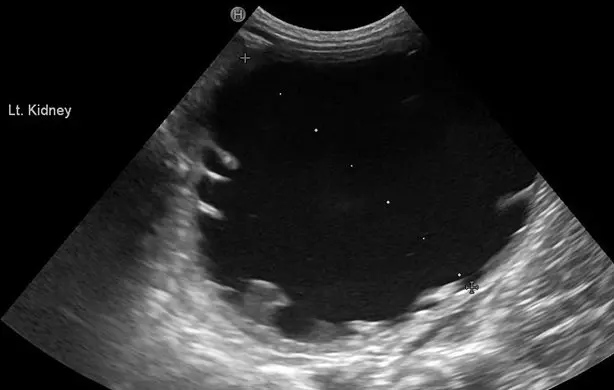
Figure 1. An ultrasound and endoscopic image of a ureterocoele in the bladder neck of a male dog with an ectopic ureter.
Ectopic ureters are the most common congenital abnormality of the urinary tract, and in female dogs tend to present with continuous urinary incontinence at a young age. However, ectopic ureters are also seen in male dogs, but tend to present and require treatment in a different way.
This article aims to outline the presentation, appropriate diagnostic tests and options for management.
The majority of male dogs with ectopic ureters will be Labrador retrievers; however, it is also occasionally seen in other breeds.
In contrast to female dogs, less than 50% of the male dogs seen in the author’s hospital with ectopic ureters present with urinary incontinence and, where this is seen, it is generally less severe than in females. This is due to the very long length of the male urethra and the lower rate of concurrent urethral sphincter mechanism incompetence.
Given that male dogs with ectopic ureters often have a very stenotic ectopic ureterovesicular junction, the remainder of these patients will present with hydroureter or hydronephrosis (or both), which is frequently identified incidentally when abdominal imaging is performed for another reason.
Other possible presentations include recurrent urinary tract infections, dysuria (frequently due to concurrent ureterocoele formation; Figure 1) or detected abdominal mass lesions (typically markedly hydronephrotic kidneys).
In female dogs, the combination of abdominal ultrasound and urethrocystoscopy has become the mainstay of diagnosing ureteral ectopia and, in the right hands, has better sensitivity/specificity than other modalities (Figure 2).
In male dogs, historically, the lower image quality of flexible urethrocystoscopy has limited its use as a primary diagnostic modality. Ultrasound may be suggestive in some cases and indeed identify the obstructive consequences (Figure 3); however, contrast advanced imaging (CT intravenous urography) likely has the best diagnostic performance at this time. The quality of endoscopic images has improved; however, the stenotic openings can still be difficult to identify.
It is also important to perform urine analysis/culture as part of the diagnostic work-up, as the presence of a urinary tract infection may increase the risk of complication after treatment. Given concurrent renal dysplasia is also seen, and given the potential for hydronephrosis, evaluation of renal function is also appropriate.
Ureteral ectopia in dogs was previously managed with conventional surgical techniques such as re-implantation or cystotomy/urethrotomy for ablation. However, these techniques were associated with very high complication rates, such as a 50% chance of stricture or stenosis of ureteral reimplantation sites. For that reason, cystoscopic laser ablation is now regarded as the preferred technique for management and is well established in female dogs (Berent et al, 2012).
In brief, the procedure involves placing a ureteral catheter or wire into the ureter under cystoscopic guidance, and then passing a laser fibre down the working channel of the cystoscope to ablate the medial wall of the intramural tunnel. This effectively moves the opening cranially, ideally to a relatively normal anatomical location.
Treatment is still indicated, even in dogs that are not incontinent, although ureteronephrectomy should be a consideration in some cases if the degree of ureteral distension/hydronephrosis is such that little material chance of any functional recovery of the kidney exists.
While endoscopic procedures are technically achievable in male dogs (Berent et al, 2008), the previously limited image quality of flexible ureteroscopes (used for male urethrocystoscopy) meant that the procedure had to be performed via a perineal approach into the urethra in many cases (Figure 4). This involves puncturing the perineal urethra, under fluoroscopic and ultrasonographic guidance, achieving wire access and then serially dilating this opening before placing an access sheath that permits passage of a rigid endoscope.
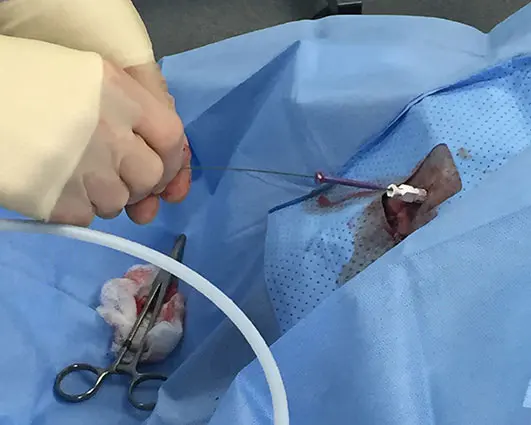
This significantly increased the complexity and duration of these procedures, and was not always successful.
Over the past five years or so, significant developments have been made in endoscopic technology, with very high-quality video ureteroscopes becoming more widely available; options for this now include re-usable and disposable scopes. These developments have revolutionised our approach to these procedures and made it realistic for intricate urinary tract procedures to be undertaken completely non-invasively via the urethra.
The author has pioneered the use of flexible urethroscopy to perform laser ablation and believes this should now be considered the preferred technique for male dogs.
Like many urinary interventions, male ectopic ureter laser ablation is performed using both endoscopic and fluoroscopic guidance (Figure 5).

Flexible ureteroscopes are generally around 8 Fr to 9 Fr (3mm) in size with a 3 Fr to 3.7 Fr (1mm to 1.2mm) working channel. While a number of lasers have been described to be effective for laser ablation, the author favours the use of a diode laser (typically 980nm with output up to at least 25W), as the continuous action reduces bleeding and tissue trauma. A laser fibre appropriately sized for the working channel of the endoscope is required.
Patients are positioned in dorsal recumbency and the area around the prepuce is clipped and appropriately scrubbed (Figure 6). The bladder is emptied and then an initial flexible urethrocystoscopy is performed, with constant irrigation of warmed fluid via the working channel of the endoscope, to confirm the diagnosis. While some cases are very obvious, in many males the stenotic opening is very difficult to see and hidden in the mucosal folds of the urethra. Equally, the prostatic ducts open in a similar area and are easy to confuse for a small ectopic opening to the untrained eye (Figure 7). A very meticulous interrogation is, therefore, required to identify the opening (Figure 8). Once this is established, a hydrophilic guide wire is inserted into the working channel and advanced through the ectopic opening into the ureter. Fluoroscopy can be used at this stage to demonstrate that the wire is indeed passing into the ureter and to chart the anatomy.



Ideally, the endoscope is withdrawn over the wire, leaving this in place during treatment; however, this is not always possible. Once the opening has been confidently identified, the laser fibre is advanced down the working channel of the endoscope and used to carefully ablate the medial wall of the ectopic ureter. In most cases, once the initial stenotic portion has been ablated, the course of the ureter is very clear due to the dilation (Figure 9). As with females, the intention is to move the opening into a relatively normal anatomical location.

With patience and experience, flexible endoscopy can be utilised for the vast majority of male dogs (more than 95%), as long as they are large enough to accommodate the endoscope (typically at least 8kg to 10kg). The procedure is rapid, and patients will generally be discharged the same day with three days of analgesia.
A significant portion (approximately 30%) of female dogs with ectopic ureters continue to have varying degrees of urinary incontinence due to presumed concurrent urethral sphincter mechanism incompetence. While the same is possible in males, in the author’s experience the vast majority (more than 95%) will be completely continent afterwards; this is an equivalent or better outcome than conventional surgery (Anders et al, 2012).
Other possible complications include acute and chronic infections and polyp formation, but these also seem to be less common than in females.
In summary, the author believes that flexible urethrocystoscopic laser ablation should be considered the preferred option for management in the majority of male dogs with ureteral ectopia. As the pioneer of this procedure in the UK, he currently sees secondary and tertiary referrals from across the country for these interventions and would be delighted to discuss suitable cases with colleagues.
Andrew Kent graduated from the University of Bristol and spent time in mixed and small animal practice before moving to The Queen’s Veterinary School Hospital in 2012. He became an internal medicine specialist in 2016 and, in 2023, joined IVC Evidensia as the clinical director of Blaise Veterinary Referral Hospital. Andy still enjoys a varied clinical caseload, but has particular interests in urinary tract disease, gastrointestinal disease and interventional radiology/endoscopy.