17 Feb 2026
Anette Loeffler, DrMedVet, DVD, DipECVD, FHEA, MRCVS examines new advice for the diagnosis and treatment of this disease in dogs – including how to reduce unnecessary antimicrobial use.
Anette Loeffler
Job Title
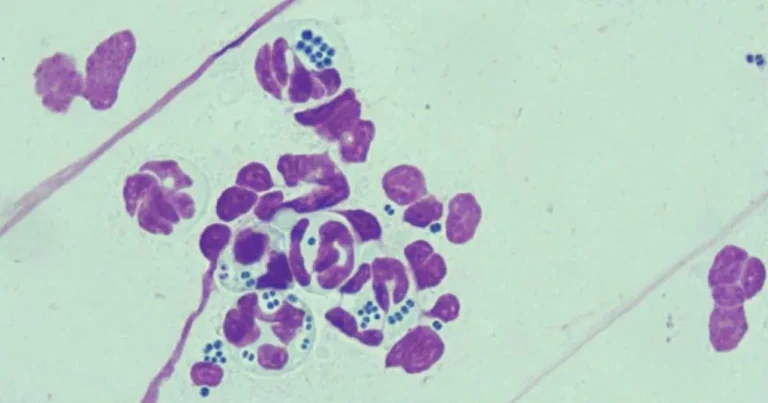
Figure 1. Large neutrophils and intracellular cocci.
Historically, staphylococcal pyoderma was easy to treat, more difficult to prevent from recurring, but overall presented few challenges to clinicians. However, since the emergence of meticillin-resistant Staphylococcus pseudintermedius (MRSP) over the past 15 years, treatment choices for some deep infections have become extremely limited.
Given the critical threat to human and veterinary medicine from antimicrobial resistance, an urgent need now exists to minimise antimicrobial prescribing and use antimicrobials responsibly to preserve their efficacy for the future. The skin provides excellent opportunities for such antimicrobial stewardship due to its accessibility for in-house diagnostic testing and topical therapy.
This review outlines developments and treatment recommendations from the recently published International Society for Companion Animal Infectious Diseases’ antimicrobial use guidelines for canine pyoderma. Guidelines are designed to provide clinicians with easily accessible evidence-based information to help with treatment decisions that maximise the chances of treatment success and, at the same time, minimise inappropriate antimicrobial use.
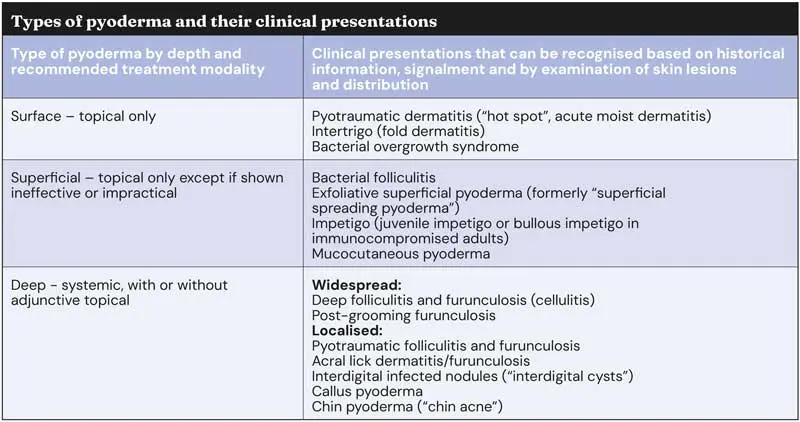
Pyoderma presents with a wide range of different clinical presentations in the dog, depending on depth of infection (surface, superficial, deep pyoderma), coat type, underlying primary causes and, likely, many unknown factors; correct identification of the depth of infection is important for choosing the correct treatment route.
The diagnostic section of the guidelines includes an overview on clinical recognition of the different types of pyoderma and places particular emphasis on the importance of in-house cytology, of investigations into underlying primary causes, and of appropriate use of bacterial culture and susceptibility testing. Cytology of lesional skin samples should be performed in every case of suspected pyoderma to confirm a bacterial cause before antimicrobial therapy is prescribed.
Cytology can be achieved in every practice setting with very little time and funding required. A rapid staining kit and a microscope suitable for examining samples under oil immersion (×100 lens for ×1,000 magnification) will allow identification of relevant features from skin samples (for example, tape strips, impression of lanced pustule or swab smears).
Finding intracellular bacterial (typically cocci within neutrophils; Figure 1) or extracellular bacteria with nuclear streaming or large numbers of actively dividing bacteria will be supportive of pyoderma, and differentiate pyoderma from Malassezia dermatitis or sterile inflammatory disease, for example. Cytological examination can also be extremely valuable for monitoring treatment responses or identifying treatment failure and drug resistance.
It is accepted these days that canine pyoderma is always secondary to an underlying primary cause. The key question, therefore, in any pyoderma consultation should always be: why did infection occur (or recur)? Investigations into such primary causes need to be an integral part of any diagnostic approach, already at the first occurrence.
Treatment success and prevention of recurrent pyoderma depend not only on treating the infection, but also on identifying and correcting or controlling these primary causes to prevent recurrence. Ectoparasite infestations and atopic dermatitis accounted for 80% of primary causes in one retrospective study, but trauma, endocrine, other systemic disease, neoplasia or keratinisation disorders should also be considered and investigated, depending on historical and clinical parameters of the case. Repeating such investigations into underlying causes at six-monthly or 12-monthly intervals, for example, is especially important in dogs that require repeated courses of systemic antimicrobials for recurrent pyoderma due to so-far unidentified primary causes.
Where allergic skin disease is suspected (but cannot be proven), anti-inflammatory treatment should be prioritised over repeated antibiotic use unless proactive, long-term topical antiseptic therapy is effective in preventing relapse.
Bacterial culture and antimicrobial susceptibility testing (BC/AST) is always recommended when systemic antimicrobial therapy is indicated to inform on drug choices and reduce the risk of treatment failure. It is also strongly recommended in all cases of deep pyoderma and when risk factors for MRSP or multidrug resistance are recognised, such as:
BC/AST is a highly valuable test that facilitates responsible antimicrobial use at multiple levels. However, given the often regrettably high cost of BC/AST, indications for laboratory testing need to be carefully evaluated and justified. BC/AST is not needed for the diagnosis of pyoderma, as even samples taken from healthy skin will most often grow bacteria, including S pseudintermedius as a common commensal in dogs (cytology is needed to confirm infection). BC/AST is also not needed if the dog is going to be treated with topicals alone (that is, any case of surface pyoderma and most cases of superficial pyoderma).
Laboratory reports on predicted susceptibilities are based on clinical breakpoints, which are designed by taking into account pharmacokinetic and dynamic information of drugs given systemically. Currently available breakpoints do not apply to the application of a drug via the topical route and laboratory results are, therefore, not meaningful for selecting topical therapy.
For surface and superficial pyoderma, strong evidence shows that topical antimicrobial therapy, as the sole antimicrobial treatment, is effective (and safe) and, therefore, the treatment of choice. Key for treatment success overall, though, will be the treatment of concurrent primary causes.
In surface pyoderma, where inflammation is well known as the main driver for microbial overgrowth, the combination of topical antimicrobials with either topical or systemic glucocorticoids has been shown to be effective in several studies, including randomised controlled settings.
Although clinical improvement may be slightly slower than with systemic treatment, improvement is usually evident within one to two weeks, while full resolution should be seen within three to four weeks. Systemic antimicrobials are never indicated in surface pyoderma and should not be used routinely for superficial pyoderma either, only for a small number of cases where topical therapy alone has been ineffective or is impractical.
Deep pyoderma represents a more serious condition due to the proximity of infection to blood vessels in the dermis and the associated risk of progression into septicaemia. Systemic antibacterial therapy is, therefore, indicated in every case. Given the greater variety of bacterial pathogens found in deep pyoderma and their more varied drug susceptibilities, BC/AST quickly becomes cost effective in deep pyoderma cases and helps to avoid treatment failures (around 40% of bacteria isolated from deep pyoderma include Gram-negatives or anaerobes compared to superficial pyoderma, with more than 90% yielding S pseudintermedius). The addition of topical antimicrobial therapy is recommended as soon as the dog is considered pain free.
The guidelines place significant emphasis on a review of the recommended duration of systemic antimicrobial therapy. Shorter courses of antimicrobials are considered less detrimental to the gut microbiome and associated health parameters.
Furthermore, a large body of evidence from human medicine is now available, including studies on skin and soft tissue infections, which support that short courses can be as effective as long courses and that historical recommendations are questionable. The review of evidence on required treatment duration by the guideline team resulted in equivocal results, mainly because treatment studies are sparse, relatively dated and not of comparable design. In the absence of good data, the guideline recommendations settled on initial prescriptions of two weeks for superficial pyoderma and of three weeks for deep pyoderma (without additional weeks beyond clinical cure and historically advised). However, these shorter initial prescriptions should be combined with scheduled veterinary re-checks, so that progress can be assessed before treatment is stopped. Fixed re-examinations while still receiving antimicrobials will allow the clinician to determine whether extended treatment is necessary (based on lesion assessment and cytology), to identify drug resistance early and, most importantly, to continue investigations and correction of primary underlying causes.
Where lesions remain after resolution of infection, based on clinical signs (for example, no more draining lesions) and cytology (absence of bacteria in representative samples), systemic antibiotics can be stopped, but treatment needs to continue with medication addressing primary causes; for example, this is frequently the case with infected interdigital nodules where the infectious component can typically be resolved with three weeks of antibiosis, but where the granulomatous – by then sterile – pathology needs to be addressed with anti-inflammatory medication to facilitate further healing.
Topical antimicrobials include active ingredients, which should be selected based on available evidence for efficacy and safety, while product formulations need to be tailored to the dog’s presenting signs, temperament and owner needs or practicalities to ensure best contact, product penetration and owner compliance.
A combination of rinse-off (shampoo) and leave-on preparations (cream, ointment, foam or spray) with at least once-daily application of one of the formulations would be a common protocol. Treatment outcomes can further be enhanced by clipping of matted hair, removing excess debris using water and wipes, ensuring adequate contact times and distracting dogs from licking off the product through play, walks or feeding.
Active ingredients are either antiseptics that by definition inhibit or kill bacteria, and can be applied to living tissue, such as skin (in contrast to disinfectants that are for use on inanimate objects). Topically used antimicrobials include molecules that are derived from microorganisms or may also be available for systemic therapy in some species. Good evidence for efficacy against staphylococci in vitro exists for a huge number of agents. However, clinical evidence, where efficacy has been demonstrated on skin, in the presence of organic material and in a clinically applicable formulation, is less abundant.
Data are available supporting use of chlorhexidine 2% to 4% in various formulations. For surface pyoderma, fusidic acid, which has excellent, narrow-spectrum anti-staphylococcal activity, in combination with betamethasone as ointment, was as effective as antibiotics and glucocorticoids given systemically.
While any agent applied to the skin can potentially cause irritation, adverse reactions are extremely rare and should be reversible once treatment is stopped. Concerns about “drug resistance” (tolerance) are occasionally raised, but no cases of treatment failure due to reduced susceptibility have been reported in human or veterinary medicine where other contributing factors could be excluded.
For systemic therapy, the guideline team grouped drugs specifically for canine pyoderma, combining considerations of efficacy based on published evidence, the importance of a drug for human medicine and clinical safety considerations in the clinical context. First-choice drugs for canine pyoderma (clindamycin, cefalexin and co-amoxiclav) have good predicted efficacy against most meticillin-susceptible Staphylococcus species, combined with a low risk of adverse clinical effects. If drugs are chosen empirically, only those three should be considered.
Second-choice drugs should only be used with BC/AST results showing susceptibility and without any of the first-choice drugs being suitable.
Second-choice agents include the fluoroquinolones (enrofloxacin, marbofloxacin and pradofloxacin) and the third-generation cefovecin. While these drugs are grouped as second-choice for stewardship reasons, tetracyclines and potentiated sulfonamides are included due to a greater risk of clinical complications (treatment failure during treatment due to the “promiscuous” exchange of small, mobile tetracycline resistance genes; for trimethoprim/sulfamethoxazole, dose-dependent keratoconjunctivitis sicca [reversible] and idiosyncratic sulfonamide hypersensitivity with potentially severe clinical manifestations are well-known risks).
Certain critically important human antimicrobials (included in the guidelines as “reserved” and “strongly discouraged drugs”) may occasionally be needed for a small number of multidrug-resistant MRSP infections. These drugs are off licence for dogs in the UK and associated with a significant health risk. If considered, specific guidelines and advice from colleagues who have used these medications should be consulted.
In conclusion, the use of in-house cytology, prioritisation of topical therapy and a consistent focus on underlying primary causes of pyoderma should be an integral part of day-to-day practice when dealing with a case of presumed canine pyoderma.
For treatment of the microbial component of pyoderma, a wide range of topical and systemic agents and products is available, supported by good evidence for efficacy. However, for successful treatment outcomes long term, antimicrobial therapy needs to be backed up by concurrent treatment of primary causes. Also, to ensure the most responsible use of the precious systemic antimicrobials, systemic drug choices are best made with the help of BC/AST results, and all efforts should be made to keep antimicrobial courses short through good clinical progress monitoring, adjunctive topical therapy and addressing the primary causes.
By taking advantage of the accessibility of the skin, clinicians have a clear opportunity to improve clinical outcomes while significantly reducing unnecessary antimicrobial use.