11 Apr 2022
Laura George looks at these common disorders/diseases seen in practice, including causes, the diagnostic process, clinical signs, as well as caring for these patients.
Laura George
Job Title
Image © Chalabala / Adobe Stock
Gastrointestinal (GI) issues (for example, vomiting, regurgitation, abdominal pain or diarrhoea) are some of the most common reasons for owners to bring their pets to the practice, and these issues may be reported as either acute or chronic in nature.
Some cases of acute GI upset – for example, vomiting and diarrhoea – will be self-limiting and resolve with minimal intervention. In other cases, intensive management and long-term treatment is needed to treat these patients.
This article will cover the clinical examination and diagnostic processes of the patient with GI issues, before examining the specific GI issues and associated clinical signs.
The first part of any clinical examination is collection of a thorough patient history from the owner, and this should start with patient signalment (that is, breed, age, sex, gender, environment), as this can provide clues to the underlying cause, before moving on to more detailed questioning regarding GI and nutritional status (Bondy Jr and Wortinger, 2012).
To gather useful information regarding the patient’s GI status, certain questions should be asked (Panel 1) and this is something VNs can assist with and may be better placed, in some circumstances, to do so – such as during nursing clinics.
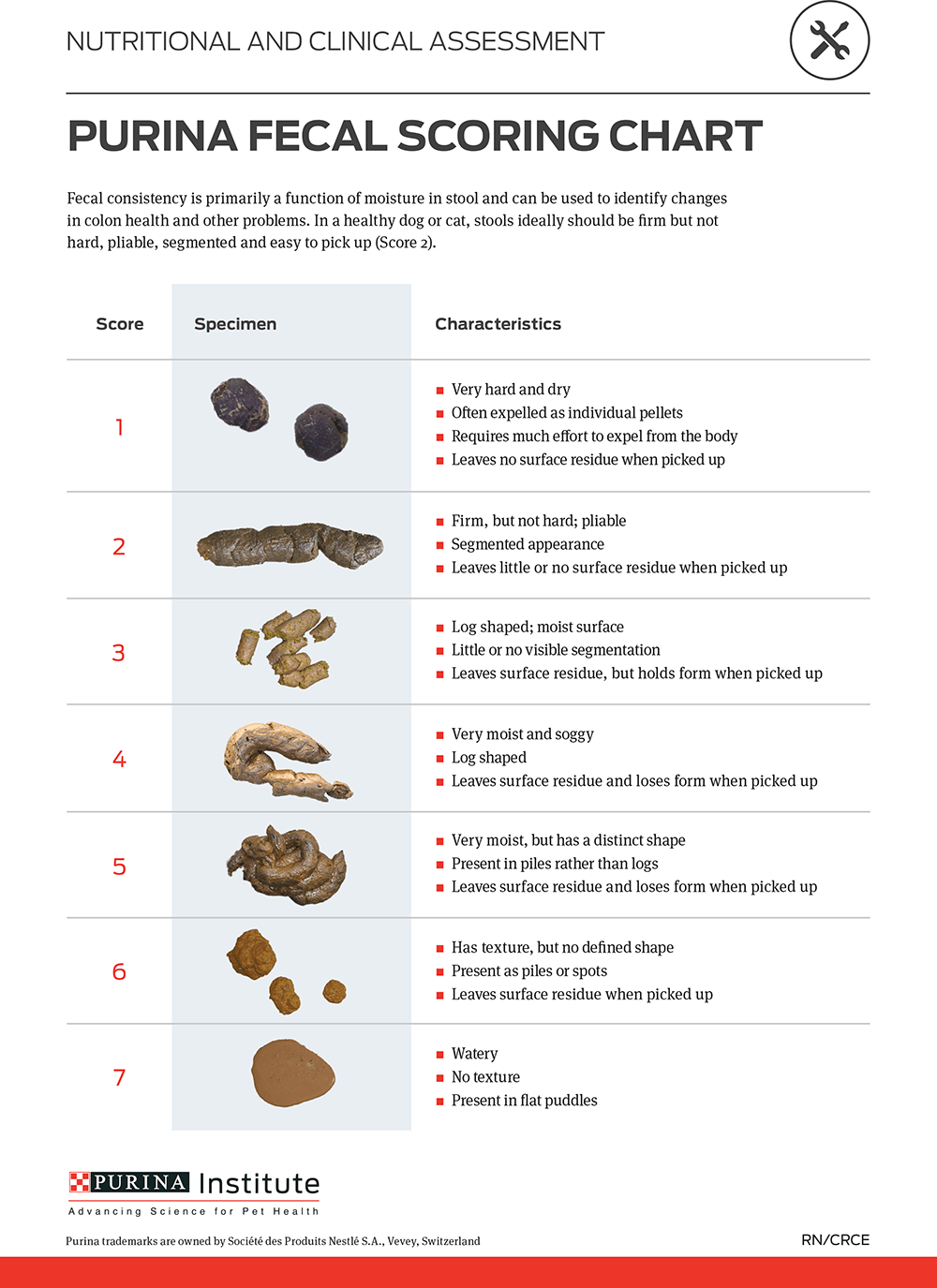
If an owner reports diarrhoea, it can be helpful to ask them to grade it using a “faecal scoring chart”, such as that offered by Purina (Figure 1).
It is also useful to differentiate between the type of diarrhoea, either small or large bowel in origin, by determining certain features (Table 1).
| Table 1. Large bowel versus small bowel diarrhoea (Sabatino, 2019) | ||
|---|---|---|
| Small bowel | Large bowel | |
| Urgency | No | Yes |
| Straining | No | Yes |
| Frequency | Usually infrequent | Usually frequent |
| Frank blood | No | Yes |
| Mucous | No | Yes |
| Greasy stool | Sometimes | No |
| Weight loss | Yes | No |
| Melaena | Sometimes | No |
| Volume of stool | Large volume | Usually small volume |
The next step is a thorough clinical examination and, although something usually performed by a veterinary surgeon, the VN can be heavily involved with this, so an understanding of the process is vital. Every clinical examination starts with general observation of the animal and parameter measurements (Panel 2). In addition, patients with GI issues may also have their abdomen palpated for abnormalities (for example, abdominal pain or presence of a foreign body/mass), and auscultation can be performed to listen for gut sounds.
Based on the information gathered and the clinical examination, the vet can localise the area of concern (the oesophagus, stomach, small intestine or large intestine), and build a problem list to guide further diagnostics and treatment.
Many different investigative tests are available that can be performed patients suffering from GI issues. Some are non-specific to GI disease, but may reveal a more generalised cause for the signs being displayed.
Basic biochemistry testing is likely to be performed in any patient presenting with GI signs, along with more specific tests guided by the examination findings:
Faecal testing may be performed in patients with diarrhoea and include:
Radiography may be useful in the case of a GI foreign body (FB), but contrast studies may be required to highlight this. If the FB is radiopaque (for example, a metallic object), it will be viewed on a plain radiograph. Alternatively, gas distension may be seen proximal to the obstruction.
Thoracic radiographs may be indicated in cases of regurgitation to rule out/diagnose megaoesophagus – these are performed conscious to reduce air artefact.
Ultrasound is regularly performed in all patients with GI issues and it allows for visualisation of the entire GI tract, and for measurement of wall thickness of the stomach and intestines, as well as allowing characterisation of the walls of these organs (that is, any mass present).
GI endoscopy is a common procedure involving the passage of a camera either through the mouth, down the oesophagus into the stomach and into the duodenum, or through the anus to examine the rectum, colon and, if able to pass the ileocolic valve, the proximal part of the small intestines. This minimally invasive procedure allows visualisation of the mucosal wall, collection of tissue samples and removal of foreign bodies (depending on size, shape and texture). If, on ultrasound imaging, the jejunum is the area of interest, endoscopy is unsuitable as this area of the small bowel is inaccessible by endoscopy. Recent diagnostic advances include videoendoscopic capsules.
The capsule is administered orally, and travels the entire length of the GI tract (including the jejunum) by peristalsis and collecting 360°C views. The capsule is then retrieved from the faeces and sent to the manufacturer, where the images are downloaded, analysed and a report created.
In certain cases surgery may be indicated to obtain a diagnosis; for example, if the issue has been localised to the jejunum, which is unreachable with endoscopy, or if full thickness biopsy samples are warranted. Surgery may also be needed to treat the cause of the GI issues, including FB removal if unable to remove via endoscopy.
Various clinical signs are associated with GI disease and the definitions of these are detailed in Table 2. A multitude of GI diseases exist, many of which are outside the scope of this article. The following is a brief overview of some of the most common diseases that VNs will see in practice.
| Table 2. Definitions of clinical signs associated with gastrointestinal (GI) disease (Bondy and Wortinger, 2012) | |
|---|---|
| GI sign | Definition |
| Anorexia | Loss of appetite. |
| Borborygmi | Rumbling gut sounds – caused by a shifting gas-fluid interface. |
| Cachexia | Loss of appetite with weight loss and muscle mass loss. |
| Constipation | Dry, hard faeces that are difficult to pass. |
| Diarrhoea | Loose, watery faeces. |
| Dyschezia | Difficulty passing faeces. |
| Dysphagia | Difficulty swallowing. |
| Haematemesis | Blood in vomit. |
| Haematochezia | Fresh blood in faeces. |
| Melaena | Black, tarry faeces due to the presence of digested blood. |
| Ptyalism | Excessive salivating. The patient may be unable or unwilling (in too much pain) to swallow, but this sign is also attributed to nausea. |
| Regurgitation | Passive expulsion of ingested contents from the oesophagus. |
| Tenesmus | Ineffective straining to pass faeces. |
| Vomiting | Forceful expulsion of material from the stomach or proximal duodenum. |
Gastritis is an inflammation of the stomach lining, and may be acute or chronic in nature.
Acute gastritis is characterised by sudden vomiting, with the vomited material containing food and/or bile, and additional clinical signs include anorexia and possibly nausea (Bondy Jr and Wortinger, 2012).
Various underlying causes of gastritis exist (Panel 3), and unless the patient has been actively observed ingesting something untoward (FB, toxin), obtaining a thorough clinical history will play a key role in the final diagnosis.
Treatment is usually supportive and symptomatic, including intravenous fluid therapy to restore any fluid deficits and provide a maintenance rate, anti-emetic medications, for example, maropitant, and withholding food for 24 hours (Bondy Jr and Wortinger, 2012). After this a bland diet can be introduced before a gradual transition back to their own diet over three to five days. If clinical signs persist or worsen, further investigations may be warranted in the form of blood tests and diagnostic imaging.
Colitis is inflammation of the colon and is the term commonly used to describe LI diarrhoea (Table 1). Stress, infectious disease (for example, Salmonella, Escherichia coli, and Clostridium), and parasites (for example, Giardia, Cyrptosporidium and whipworm), and inflammatory bowel disease (IBD) are all potential causes.
Dietary indiscretion may also result in a bout of colitis. Regardless of the aetiology, the result is a reduced water absorption and ability to store faeces in the colon; hence the small, frequent amounts of diarrhoea (Defarges, 2020).
Diagnosis is based on clinical history, faecal testing and rectal examination. Further diagnostics, including faecal culture, abdominal ultrasound, colonoscopy and biopsies, may be warranted depending on the history, clinical findings and response (or lack thereof) of medical management.
Patient hygiene is crucial in cases with colitis. If the patient is suspected/confirmed to have an infectious cause, they should be barrier nursed appropriately and correct personal protective equipment should be worn. Some infectious causes are zoonotic, so protecting personnel is important to prevent contracting the pathogen.
Treatment should focus on infectious causes first (if applicable), followed by diet alterations. Feeding a diet with increased fibre can improve diarrhoea, but may take some time and rarely resolves the issue completely (Defarges, 2020).
Novel protein diets (truly hypoallergenic diets) are diets including a single protein source and can control the signs of colitis, and many commercially available options are available.
Hydrolysed diets are another option, and these work by disrupting the protein structure, removing allergens and preventing immune recognition (Defarges, 2020).
If dietary change alone does not resolve the colitis, antibiotics may be prescribed, but these are not the first line of treatment in patients with it, unless an infectious cause has been identified.
Metronidazole is commonly used in cases of colitis. Anti-inflammatory medication may also be warranted as an adjunct to dietary management and metronidazole if clinical signs persist – sulfasalazine, prednisolone and azathioprine are all commonly used options (Defarges, 2020).
Long-term use may lead to clinical side effects being observed, including keratoconjunctivis sicca, when using sulfasalazine (Defarges, 2020), or the muscle wastage, polyuria, polydipsia and polyphagia seen with glucocorticoids.
Faecal transplantation is a relatively new treatment for colitis, but may be a suitable option in cases of refractory colitis.
GI ulceration is characterised by sudden onset vomiting with haematemesis.
Ulceration occurs when the gastric mucosal barrier is disrupted. This defence mechanism is responsible for ensuring the GI mucosa remains healthy. When disrupted, either due to direct injury, reduced blood flow, increased gastric acid secretion or shifts in protective prostaglandins (Blois, 2020), ulceration can develop.
Hepatic disease and uraemia are both potential causes for GI ulceration. NSAIDs are implicated as a cause of GI ulceration as they can inhibit the protective prostaglandins. COX-2 inhibitors are thought to have less of an effect on the protective prostaglandins, but this is still a risk (Blois, 2020).
Primary GI neoplasia may also result in GI ulcer formation due to local effects of the tumour. Abdominal ultrasound in these patients may reveal mucosal lesions or the presence of a mass in cases of neoplasia. Free abdominal gas may also be observed if the ulcer has perforated.
Endoscopy allows for identification of lesions/ulcers in various regions of the GI tract, and superficial biopsies can be collected to try to determine the underlying aetiology. It is important to note biopsies must be collected from the periphery of any lesions due to the risk of perforation (Blois, 2020).
Primary treatment is aimed at the underlying cause, but adjunctive treatments may be necessary to aid ulcer healing and patient comfort. Decreasing acid secretion is important to prevent further mucosal damage: histamine-2 receptor antagonists (for example, famotidine and ranitidine), and proton pump inhibitors (for example, omeprazole) are options, with the latter being the superior option (Blois, 2020).
Sucralfate is another drug commonly used; however, no evidence supporting its use exists (Blois, 2020). If using, it is important to administer it one to two hours apart from food/other drugs as it can inhibit the absorption of these.
If the ulcer has perforated, immediate surgery is required to resect the ulcerated area. This option may also be considered if medical management has been unsuccessful.
IBD is a syndrome caused by a reaction to a chronic irritation, and the exact mechanisms of IBD are not fully understood. This syndrome is multi-factorial and complex, the discussion of which is outside the scope of this article.
IBD is a diagnosis of exclusion and not a single test exists that can rule in/out this condition. Most patients will have a history of chronic vomiting and diarrhoea and will undergo investigation, including GI biopsies (either endoscopically or surgically), folate and cobalamin testing and faecal analysis.
IBD is managed rather than cured, and the patient may be treated with a combination of dietary change and medication This is generally tweaked to the individual patient.
Novel protein and hydrolysed diets are commonly used, and an exclusive diet trial may be the first recommendation. This involves feeding only the prescribed diet for six to 12 weeks to assess response. Some cases may then be managed on diet alone; it is important to support owners during this time, and they must understand that no other food or treats can be given.
Adjunctive treatment may be needed and these are similar options to those prescribed for colitis, including anti-inflammatories and antibiotics. De-worming is also recommended. If folate and/or cobalamin levels are disrupted, supplementation can be provided – folate in the form of tablets and cobalamin in the form of a subcutaneous injection.
Many other GI disorders/diseases exist, which will have their own specific diagnostic and treatment plans, including:
GI issues in small animals include a wide range of clinical signs, diseases and disorders, and this article is only able to provide a brief overview of these.
The collection of an in-depth clinical history and performance of a thorough clinical examination is key in localising the issue to a specific part of the GI tract, along with guiding appropriate investigations and interventions, and the VN can play a key role in both of these areas.