25 Jul 2022
In a new series, Gerardo Poli explores the common causes of hyperkalaemia and how to manage this using fluid therapy and medications.
Gerardo Poli
Job Title
Hyperkalaemia occurs when serum potassium concentration exceeds 5.5mmol/L.
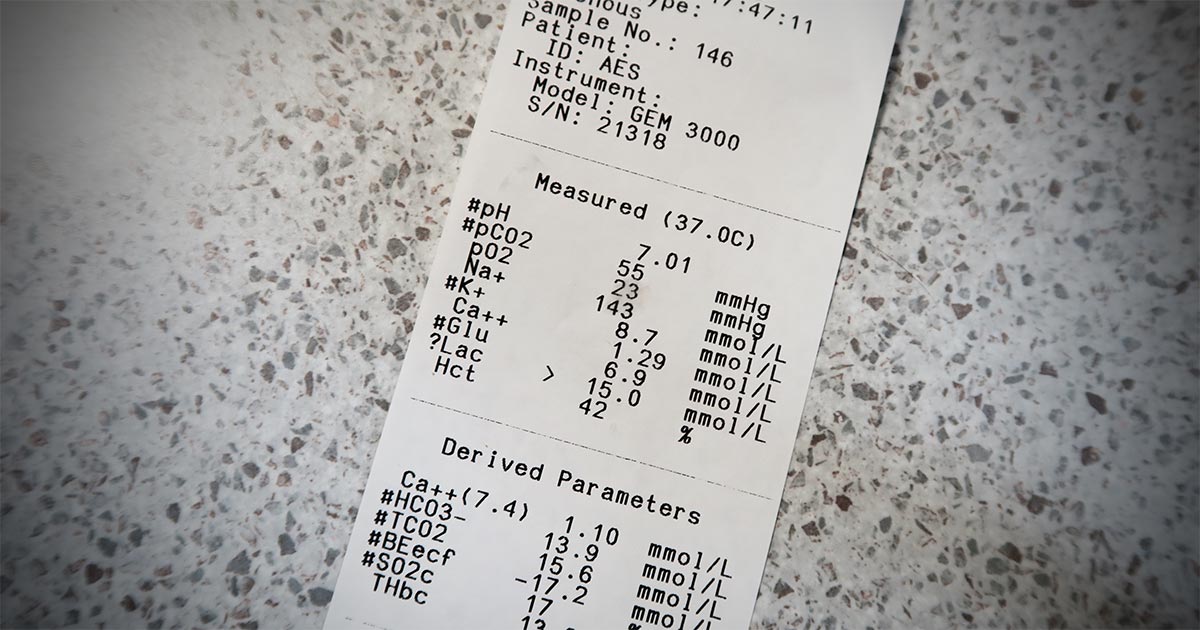
Hyperkalaemia is a relatively common electrolyte abnormality encountered in the clinic and always requires immediate attention, as myocardial toxicity can occur when serum potassium concentration gets sufficiently high (exceeding 5.5mmol/L).
Hyperkalaemia causes clinical signs due to its effect on the resting membrane potential. The increase in potassium causes depolarisation of this potential, which, in effect, causes the resting cell membrane to be less negative.
Initially, this results in an increased excitability of the membrane so that a smaller stimulus is required to stimulate the cell. However, if the resting membrane potential decreases to the point where it equals – or is less than – the threshold potential, repolarisation cannot occur and results in a cell no longer excitable.
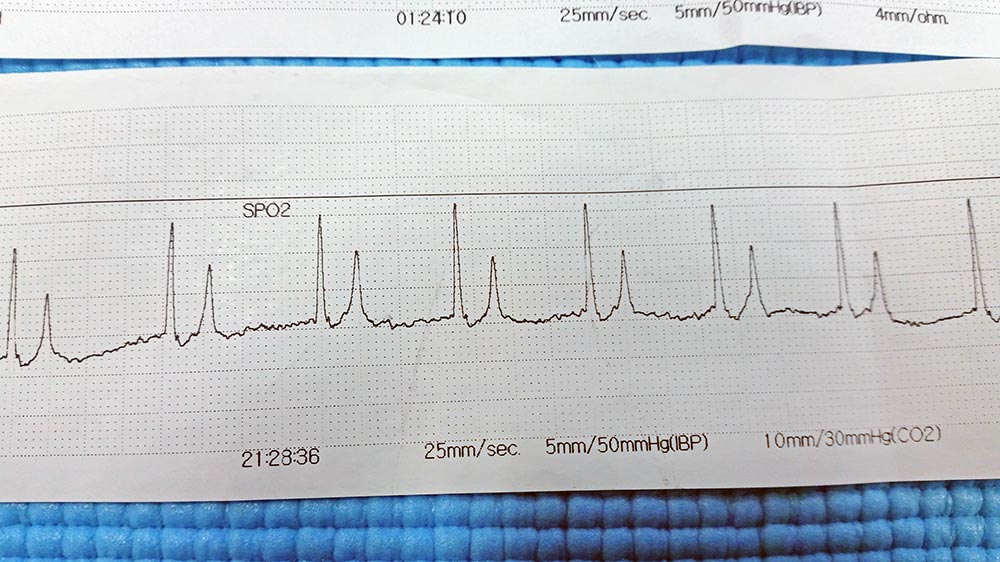
In essence, the overall effect is a reduced difference between the resting membrane potential and threshold potential, leading to the classic changes seen on ECGs – loss of P waves and peaked T waves, eventually leading to bradycardia.
Clinical signs of hyperkalaemia is concentration-associated and include:
A potassium serum concentration more than 5.5mmol/L is considered mild, more than 6.5mmol/L to be moderate and more than 9mmol/L to be severe. Theoretically, myocardial toxicity occurs when the serum concentration exceeds 7.5mmol/L.
Despite these cutoffs, the severity of clinical signs is not well correlated with the actual potassium serum concentrations in clinical patients. Therefore, myocardial toxicity should always be suspected with any animals with more than 6.0mmol/L.
ECGs are essential in these patients. They will show:
The most common causes for hyperkalaemia are reduced excretion, hypoadrenocorticism and redistribution from the intracellular fluid to the extracellular fluid:
Less common causes of hyperkalaemia include medications and artefacts. These drugs include angiotensin-converting enzyme inhibitors, trimethoprim and potassium-sparing diuretic agents.
Other less common causes of hyperkalaemia, or rather pseudohyperkalaemia, include artefact from a haemolysed blood sample, thrombocytosis and extreme leukocytosis.