24 Mar 2026
Kathryn Patel BSc(Hons), BVetMed(Hons), CertAVP(G-SAS), CertVBM discusses spotting this disease early and in younger dogs in the third part of the series promoting this year’s VOACON.
Kathryn Patel
Job Title
Mild, subtle lameness is challenging to identify for owners and the clinical team in young, active and exuberant patients.
Osteoarthritis (OA) is a common painful and progressive condition that involves degenerative changes affecting the entire synovial joint. It is frequently regarded and discussed as a disease of the elderly, with the average age of diagnosis being 10.5 years (Anderson et al, 2018).
However, awareness of its significance in young pets is increasing. A prospective study of 123 dogs found that 49 dogs (40%) had radiographic signs of OA by the age of four, with bodyweight, body condition score and age being positive predictive factors. Of those affected dogs, 29 (around 60%) had clinically detectable joint pain.
Owners had recognised mobility impairment (assessed by LOAD score) in around half of those that had joint pain recognisable by vets – yet only two dogs of the cohort had ever received any treatment for joint pain (Enomoto et al, 2024).
Yet, young dogs do not necessarily have mild OA; extreme breed conformations, genetic susceptibility and inappropriate nutrition can spell developmental joint disease and abnormal wear even in juvenile joints, so even before skeletal maturity OA may be moderate or severe.
Meanwhile, more normal dogs with few or well-managed risk factors may develop mild OA much later in life, so age is not a good proxy for disease stage. Furthermore, classification of disease – as mild, moderate or severe – does not necessarily match the patient’s experience of pain or disablement (Cachon et al, 2018).
So, why do we wait to treat? OA occurs in joints following some abnormal wear or insult, and where conformational abnormalities are present, leading to altered joint mechanics, signs may begin without any significant history of trauma.
Following joint insult, inflammatory cytokines are released which disrupt joint tissues and begin a cascade of deleterious effects on the whole joint organ, including cartilage, subchondral bone, synovium, joint capsule and local ligaments, muscles and tendons.
Secondarily, repetitive stimulation of neural pathways leads to peripheral and central sensitisation and pathological experience of pain, with resultant loss of function and impact on muscle strength and condition, proprioception, and adiposity – all of which perpetuate abnormal joint movement and contribute to further insult. Therefore, with ongoing uncorrected inflammation and abnormal mechanical wear, damage snowballs and total organ failure becomes inevitable, leading to common perceptions that OA treatment must be lifelong and OA is irreversible and incurable.
However, like all biological tissues, joint tissue has some capacity to repair. With appropriate intervention to disrupt inflammation and mechanical trauma before bone and cartilage changes become established, other factors such as synovial inflammation, nervous system sensitisation and muscle weakness are completely reversible, and the bone and cartilage changes can be halted or dramatically slowed. Therefore, proactive and positive intervention in early disease stages has the potential to dramatically alter the quality of life of affected animals (Cachon et al, 2018).
The first problem is recognition of early, mild or young patient OA. In all cases, development of secondary muscular changes leading to characteristic gait abnormalities usually depended on for diagnosis may be reduced or absent. Fit or young animals frequently have a high ability to make movement adaptations to compensate for pain caused by performing activities of daily living, which require a different approach to recognise (Lascelles et al, 2017); for example, a patient may sit “side-saddle” rather than “square” (Figure 1), offer a “lie down” when asked to “sit”, or always lift a forelimb when eating from the ground. Such activities can be interpreted as character traits and even considered charming by pet owners. Subtle lameness is difficult to identify for owners and the clinical team when puppies are exuberant.

Developmental disease can cause clinical signs while character traits are still developing – leading to perception that a pet is, for example, lazy or not playful, anxious, or afraid of stairs or the car, when in fact the behaviours seen are caused by pain associated with certain movements. Therefore, to detect such changes, veterinarians should seek to understand how pets behave at home and always keep an open mind to the possibility of pain underlying any behaviours reported.
With practice, a basic orthopaedic examination incorporating joint manipulation and palpation of major muscles groups for tenseness or spasm can be included in every routine clinical examination within just a couple of minutes.
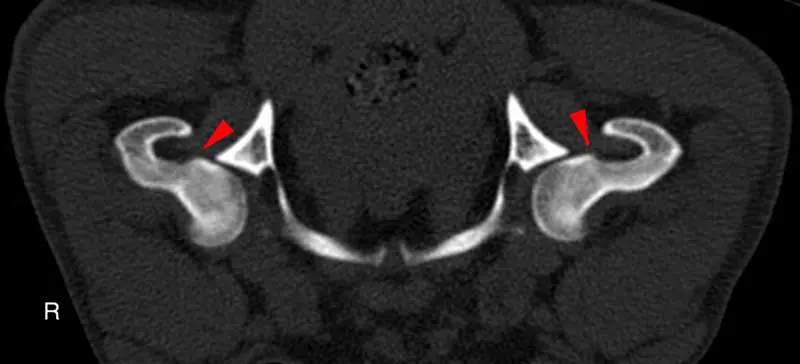
Risk assessment of all patients in for routine appointments will help to identify those that are most likely to have or develop degenerative joint disease. Risks include breeds with a genetic predisposition for OA, working and sporting dogs, dogs with a history of joint trauma or joint surgery, those that have high adiposity, or those entering senior life stage. Patients with risk factors but no symptoms may be regarded as having “pre-clinical” OA and, therefore, it is appropriate to closely monitor for development of discomfort or functional changes that could signal the onset of clinical OA, to ensure prompt intervention if needed. Diagnostics at an early stage of OA has been shown to be challenging. Radiography detects changes later than imaging such as CT, while MRI can detect even earlier changes and is the first imaging modality to be able to directly image cartilage (Figures 2 and 3; Jones et al, 2022).
Treatment at this stage should be aimed at caregiver education, mitigation of specific risk-factors when possible (such as through home adaptations, exercise modification and weight/muscle optimisation) and tailored supportive nutrition (Cachon et al, 2023).

Treatment of OA usually focuses on managing pain, which is essential for welfare. However, without addressing the underlying pathology, a risk exists that symptoms are simply masked and degeneration continues to progress. Therefore, treatment protocols must address pain while prioritising control of inflammation and incorporating targeted physical therapies to strengthen joints for normal movement, reduce adiposity and maintaining or increasing joint range of motion, to reduce future disablement.
Ideally, patient-specific OA care plans should be developed for completion at home by a qualified veterinary physiotherapist or other suitable paraprofessional, and practitioners who wish to provide modern high-standard OA care should work to build positive referral relationships with local providers to facilitate smooth handover and ongoing engagement in case progression.
In addition, nurse-led mobility clinics are an excellent opportunity to provide education on breed, lifestyle and life stage-appropriate exercise, weight management, and modifications to the home environment while offering a touch point for ongoing clinical assessment and communication on case progression to ensure treatment plans can be revised if needed.
Expert consensus guidelines recommend treatment for a minimum of four weeks at label dose to control the inflammatory cascade and reverse wind-up (Cachon et al, 2023).
NSAIDs have long been the cornerstone of anti-inflammatory and pain management, and remain an excellent first-line treatment option. Historically, vets have been resistant to use long courses of NSAIDs due to concerns about gastric, renal and hepatic side effects, and client compliance may be low due to concerns about cost, side effects or misunderstandings about treatment goals.
The category has seen significant innovation over the past 15 years, including increased COX selectivity, tissue selectivity, non-COX inhibiting molecules and long-acting preparations, in addition to the publication of various guidelines and consensus documents around safe use (Cachon et al, 2023; Innes et al, 2010; Taylor et al, 2024). A further licensed treatment option has been available since 2019 in the form of anti-NGF monoclonal antibodies. Their licensed indication is for the alleviation of pain associated with OA, not anti-inflammation, and anecdotal reports exist of non-target joint degeneration in a small number of long-term treated individuals, with a causal link speculated rather than proven (Farrell et al, 2025). This may make them a less rational selection in young patients without other complicating factors, but a compelling proposition where the need exists to control pain in patients that cannot tolerate NSAIDs.
For managing mild OA, long-term dependence on centrally acting analgesics is rarely required. Furthermore, treatment plans should prioritise licensed pharmaceuticals, as off-label drugs typically lack the robust evidence for both efficacy and safety that on-label options provide. In engaging a proactive approach to treating OA earlier, the capacity to improve the lot of affected patients is huge. However, with early treatment must come the understanding by both caregiver and clinical team that the disease is not a linear progression, but a dynamic chronic illness with periods of remission and acute flares (Carmichael and Allan, 2025).
For long-term success, each flare must be managed proactively, but it is also possible and appropriate to aim to move patients back to stable disease or remission and decrease treatments when tolerated. Through doing so, cost and risk may be minimised, and quality of life maximised, with the ultimate possibility to significantly delay or altogether avoid major disablement.