7 Apr 2026
Andrea Vila Cabaleiro DVM, AFHE, MRCVS, Dan O’Neill MVB, BSc(Hons), GPCert(SAP), GPCert(FelP), GPCert(Derm), GPCert(B&PS), PGCertVetEd, FHEA, MSc(VetEpi), PhD, FRCVS and Ella Fitzgerald MVB, CertESM, MVetMed, DipECVDI, MRCVS discuss recent advice given on nasoesophageal and nasogastric application, using real-life case examples.
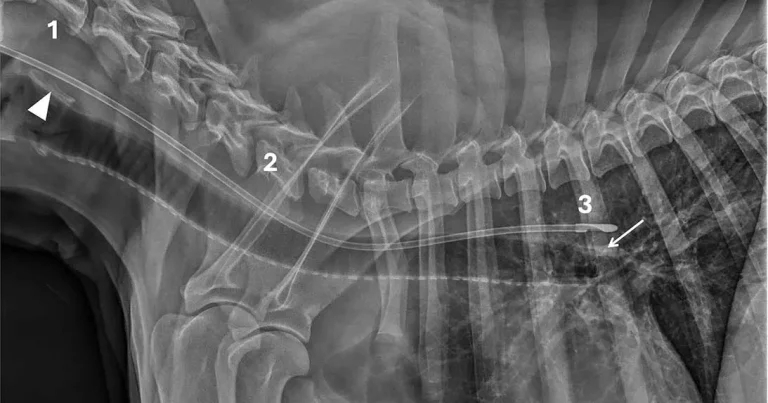
Figure 1. Case one.
Nasoesophageal and nasogastric tube feeding are essential for short-term enteral nutrition in anorexic or critically ill dogs and cats. However, inadvertent tube placement into the trachea can lead to life-threatening complications, including aspiration pneumonia, pulmonary haemorrhage or pneumothorax.
While radiography has been the recommended standard for confirmation, lack of standardised interpretation methods has limited the reliability of results – especially among first-opinion practitioners.
A new multi-institutional study, published in Veterinary Radiology and Ultrasound, introduces and validates simple, evidence-based radiographic guidelines that dramatically improve accuracy and confidence (Vila Cabaleiro et al, 2026). Application of the new guidelines by interpreters of varying experience for 256 radiographs (129 oesophageal, 127 tracheal placements) boosted correct identification from 82.1% to 95.8% (p<0.001) and reduced “uncertain” calls from 14.1% to 2.4% (p<0.001) in pre-guidelines versus post-guidelines.
This article will outline the new radiographic guidelines in detail, provide a simple protocol for taking the radiograph, and demonstrate how to apply the three-point checklist through several real-world case examples.
The guidelines are designed for quick and feasible use in everyday practice, using a single lateral radiograph including the larynx and the thorax. Avoiding the need for multiple views supports their use in busy clinics where time and patient restraint are limited. The study achieved high post-guideline accuracy (95.8% overall) with just one lateral projection.
Assess the tube against these criteria for correct oesophageal placement:
In practice, criteria two and three are essential for concluding correct tube positioning. If the tube lies dorsal to the carina (criterion three), this implicitly confirms incomplete superposition with the tracheal lumen (criterion two). Therefore, when criterion three is fulfilled, both criteria two and three are met, allowing confident confirmation of oesophageal placement.
Criterion one becomes necessary when the tube does not reach the carina and appears completely superimposed on the trachea. In this situation, assessment at the level of the larynx is required to determine tube location.
A tube passing dorsal to the lamina of cricoid cartilage indicates correct oesophageal placement, whereas a tube passing through the laryngeal lumen confirms incorrect tracheal positioning. For this reason, the larynx should be always included in the radiographic field when assessing nasoesophageal and nasogastric tube placement.
To support adoption of the new radiographic guidelines, a clear, user-friendly infographic* has been developed to guide veterinarians through the three key steps. As use of these guidelines increases, ongoing evaluation will help assess their long-term effect on clinical outcomes, with the aim of promoting safer and more consistent care for hospitalised dogs and cats across veterinary settings.
To identify the landmarks in the radiographs in Figures 1-5, arrowheads indicate the lamina of cricoid cartilage of the larynx (when included), and arrows show the dorsal wall of the carina. Additionally, numbers highlight the three criteria and landmarks: (one) larynx, (two) tracheal lumen, and (three) carina.
This lateral cervical and thoracic radiograph (Figure 1) of a dog includes the larynx and shows:
Laryngeal cartilages tend to mineralise in older dogs and occasionally in younger large-breed dogs, as in this case, with the lamina of cricoid cartilage typically the most apparent.
Interpretation. Correct oesophageal placement. All criteria were met, so the tube was safely positioned for feeding.
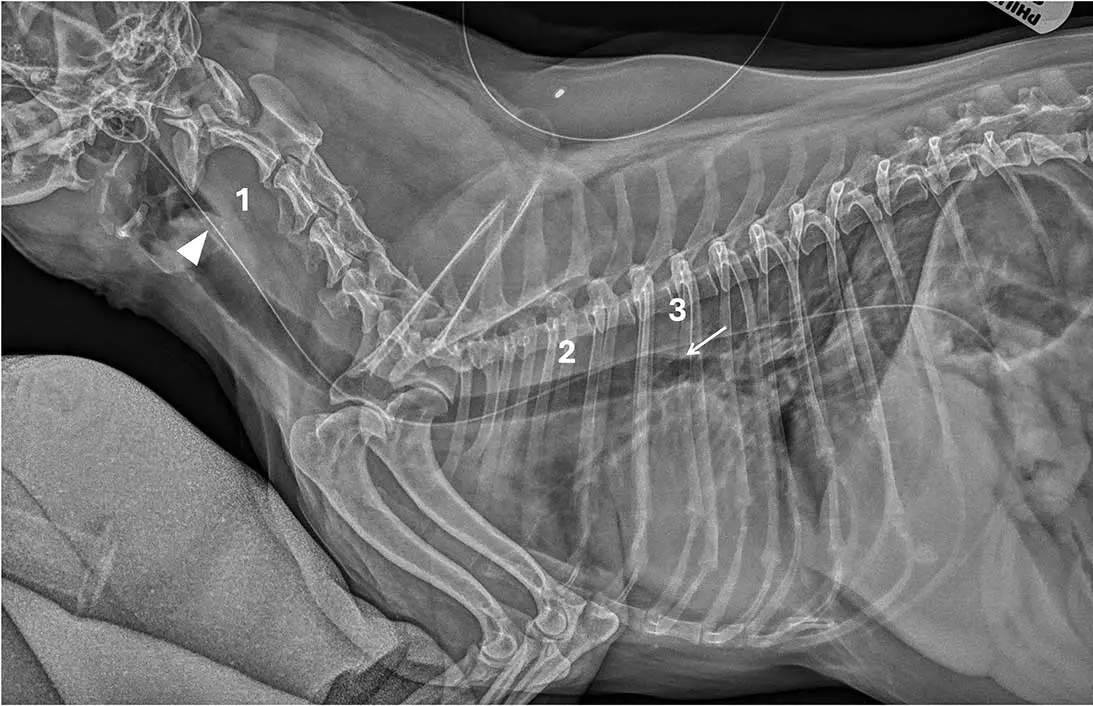
This lateral cervical and thoracic radiograph of a dog includes the larynx (Figure 2). The tube is superimposed over the laryngopharynx (1) and tracheal lumen, passing through the laryngeal lumen (arrowhead), the rest of the tracheal lumen (2) and extending to the carina (3; arrow) before following a caudodorsal bronchial path.
Interpretation. Incorrect tracheal placement. None of the three criteria are met, as the tube does not pass dorsal to the lamina of cricoid cartilage or the carina, and it completely overlaps the tracheal lumen throughout its course. The tube was immediately removed and correctly repositioned.

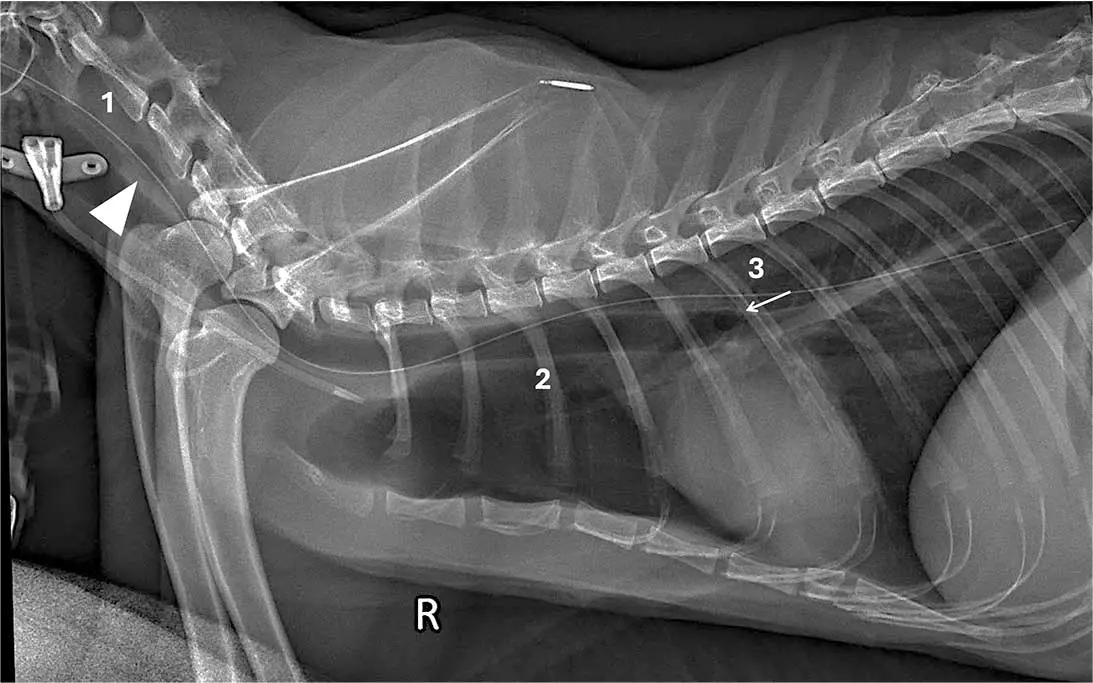
This lateral cervical and thoracic radiograph of a dog was obtained with the head rotated (Figure 3). As a result, the atlas is rotated, with the hyoid apparatus and tympanic cavities not superimposed. Therefore:
If the tube has not reached the carina, assessing its position in relation to the larynx may be safer than further advancing the feeding tube further. This case highlights the importance of achieving optimal patient positioning for radiography.
Interpretation. Correct oesophageal placement. At least criteria two and three were met; therefore, the tube was safely positioned for feeding.
This lateral cervical and thoracic radiograph of a cat includes the larynx (Figure 4), showing:
Interpretation. Correct oesophageal placement. All criteria were met, indicating that the tube was safely positioned for feeding.
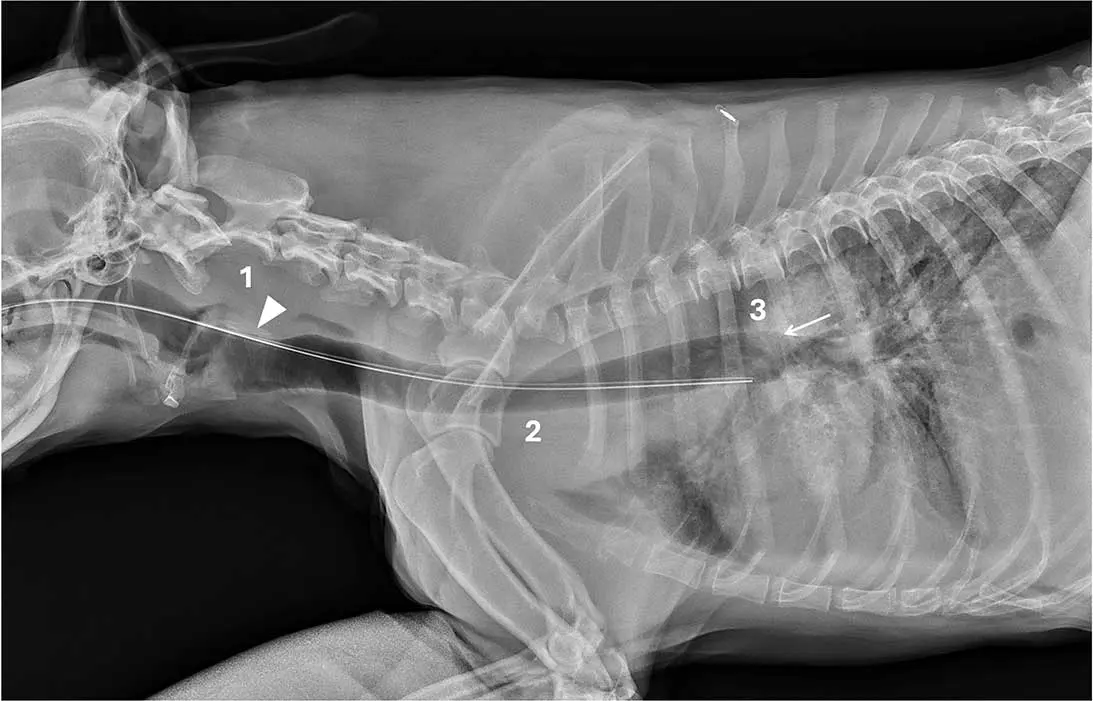
This lateral cervical and thoracic radiograph of a dog includes the larynx (Figure 5).
The feeding tube passes through the laryngeal lumen (1; arrowhead) and is superimposed over the nasopharynx, laryngopharynx and tracheal lumen (2), and it does not reach the carina (3; arrow). As the tube fails to reach the carina, inclusion of the larynx is essential to increase confidence in tube localisation.
Interpretation. Incorrect tracheal placement. Criteria one and two are not met, as the tube does not pass dorsal to the cricoid cartilage lamina, and completely overlaps the tracheal lumen throughout its course.
Criterion three cannot be used because the tube does not reach the carina. The tube was immediately removed and correctly repositioned.
These straightforward, evidence-based guidelines transform radiographic tube checks, making them more reliable and consistent for specialists and non-specialists, alike.
Do not underestimate the value of including the larynx in the radiographic field: it serves as a crucial checkpoint – particularly when the tube does not reach the carina.
If a radiograph does not clearly show that the required criteria are met, or if patient positioning or radiographic parameters are suboptimal, a repeat, optimised radiograph should be obtained before tube use. This quick three-point checklist can significantly reduce the risk of serious, potentially life-threatening complications associated with misplaced feeding tubes and can make a critical difference to patient safety.
Andrea Vila Cabaleiro graduated from the University of Santiago de Compostela (Spain) in 2017. After completing two rotating internships and earning a certificate in diagnostic imaging, she moved to the UK to work in a large first-opinion hospital. Andrea then completed a diagnostic imaging internship at The University of Edinburgh, followed by three months in the diagnostic imaging service at North Downs Specialist Referrals. She subsequently joined the RVC as a diagnostic imaging fellow and resident.
Dan O’Neill graduated from University College Dublin, followed by 22 years in general veterinary practice and 15 years in academia. With more than 190 peer-reviewed papers, he is now professor of companion animal epidemiology at the RVC and co-leads the RVC VetCompass programme. Dan is committed to promoting practice-based research to build more practical, generalisable and meaningful evidence bases that contribute to real-world improvement in animal welfare.
Ella Fitzgerald graduated from University College Dublin in 2008, then worked for five years in mixed and small animal practice in Ireland and the UK. She completed two internships and a three-year diagnostic imaging residency at the RVC in 2017. Ella is currently working remotely as part of the radiology team at the RVC and consultant radiologist for Antech Imaging Services, while also providing ultrasound services for her local first opinion practice in County Kerry.