21 Apr 2026
Ross Allan BVMS, PGCertSAS, MRCVS explains how the changing landscape of veterinary medicine affects the way clinicians approach this chronic condition.
Ross Allan
Job Title
Image: Chalabala / Adobe Stock
Canine osteoarthritis (OA) has been identified as the top chronic condition requiring improvements in its care to be prioritised. It has the largest impact on welfare based on assessment of factors including frequency of occurrence, requirement for review in primary care and the chronicity of medical management (Summers et al, 2019).
OA can also serve as a model for how to improve management of chronic diseases more broadly and it is a valuable condition to start with. One report stated the canine OA pharmacological market is valued at US$2.7 billion in 2026 and projected to reach US$4.1 billion by 2036, reflecting a compound annual growth rate of 4.2% (Future Market Insights, 2025).
The author’s opinion is that this figure is likely conservative. Pharmaceutical companies continue to develop and launch new products (Pye et al, 2022) as well as non-pharmaceutical, non-surgical treatments (Pye et al, 2024).
Many companies are open in their ambitions. Librela at launch was anticipated by Zoetis company leaders as a single product with potential to be its “next billion-dollar franchise” (Zoetis, 2024). Animalcare, in its 2024 annual report, highlights “arthritis” [sic] as being one of four highest “lifetime value” clinical conditions, and states that its product Daxocox is “poised for continued growth in the expanding osteoarthritis pain market” (Animalcare, 2024).
Does the clinician in the consult room consider these factors when they meet their next OA patients? Or is OA instead still seen as a simple diagnosis, warranting a brief explanation, easy treatment and perhaps a less than engaged long-term management plan?
One market research survey of 200 vets, quoted as being performed by Pfizer Animal Health in 1996, described OA as affecting as many as 20% of dogs older than one year old (Johnston, 1997), and in another report radiographic evidence of degenerative joint disease was evident in 90% of cats older than 12 years (Hardie et al, 2002).
High figures of reported prevalence, which do vary by methodology and population, mean an undoubted opportunity exists to improve OA clinical management and, at the same time, improve commercial performance and reinforce our professional credibility.
The Institute of Medicine defines high value clinical care as “the best care for the patient, with the optimal result for the circumstances, delivered at the right price” (Korenstein, 2015).
This definition encapsulates the essence of being a good vet, emphasising the fundamental importance of the patient-client perspective and the importance of cost, in the sense that the best care is delivered as economically as possible.
If, in veterinary medicine, many of us share a similar view, what opportunities exist for us to start towards this destination in OA management?
This article will outline why change is needed, not only for patients but also for the veterinary professions themselves. It will outline why, with the current review of the Veterinary Surgeons Act, and other changes in the wider profession, the need for the collective professions to look inwards at what we do, and agree how and what we choose to judge clinical success, can empower the professions to flourish and accelerate an increase in high-value, effective care for OA and veterinary care more broadly.
Our veterinary professions face numerous challenges: the staffing issues remaining as a legacy of Brexit and the pandemic, changes in the professions’ demographics and debt, the ongoing CMA investigations and now the proposed reform of the Veterinary Surgeons Act.
Alongside this, the economic environment we find ourselves in has dramatically changed: we are no longer in the land of low inflation and 0.25% interest rates.
These factors have led to challenging conversations within the vet profession and consulting rooms, yet most of the profession remains optimistic. Many of the external, “once ever” factors have happened, are in the past and – in the author’s personal opinion – things seem a little calmer. So, as we approach the end of the 2020s, might this decade be bookended by the “car park consults” of the pandemic and our professions’ emergence into a new professional landscape?
Prescribing and dispensing medications is a mainstay of practice, but it is not only that. “The responsible use of veterinary medicines for therapeutic purposes is one of the major skills of a veterinary surgeon.” (As stated in the RCVS Code of Professional Conduct for Veterinary Surgeons); could this be extended to also being “…crucial to animal welfare and the maintenance of public trust”?
Over the next few years, the professions themselves need to be increasingly conscious of the ecosystem we are within. Commercial responsibilities to our employers and businesses, as well as those that supply us, does influence us, and denial of this is foolish.
Awareness should serve as a catalyst to help us define “success” as a means of reinforcing our professional obligations.
The UK Government’s current consultation on the reform of the Veterinary Surgeons Act is another opportunity.
Factors being discussed include:
It is not coincidental that this review is occurring now. As the BVA succinctly stated: “The current act was designed for a different era. Nearly 60 years later, more than half of UK households now have a pet, technology has changed dramatically, and the way vets care for animals has been transformed”.
Of the possible changes, one proposal is suggesting changes in the legislation surrounding vet-led teams, which comes with potential to have a significant impact on our daily care, including OA management. Two documents from the RCVS, both titled, “Recommendations for future veterinary legislation”, outline possible reforms that could impact on the care we provide – specifically how we provide it.
Their theme is the need to develop regulation to encompass wider vet-led teams: “[Appropriately-regulated] professionals, including veterinary nurses, working under the direction of a veterinary surgeon, to protect animal health and welfare”. Another prior RCVS council recommendation to increase the role of veterinary nurses in the induction and maintenance of anaesthesia via reform of Schedule 3, enabling them to “assist in all aspects of anaesthesia under supervision”; therefore, increasing utilisation of veterinary nurses while freeing up veterinary surgeons’ time.
Additionally, the RCVS has previously explored the risks and opportunities of a “VN prescriber” role that could allow VNs to prescribe certain routine medicines that are currently restricted to veterinary surgeons (RCVS).
These reforms might seem to currently be far off, but let us start to prepare for the new tomorrow.
Costs are likely to be one reason that human health is far ahead of veterinary in pre-defining the “success” of their OA treatment and quality indicators which define what this is.
Human OA affects more than 7% of people globally (528 million people), with a higher prevalence in countries with established market economies and older populations. In these countries, the “cost” to the country is between 1% to 2.5% of gross national product, equating to an average annual cost of OA for an individual person being between US$700 to US$15,600 (£520 to £11,600; Leifer et al, 2022). In 2013, in America alone, the cost of medical expenditure for OA was estimated at US$139.8 billion (£103.9 billion), while the total arthritis-attributable medical expenditures and earnings losses were US$303.5 billion (£225.6 billion; Murphy et al, 2018).
“Framing” these costs, while GDP and gross national product differ, this means that every year most advanced economises spend on OA a figure not greatly dissimilar to what NATO countries are expected to spend on defence.
Quality indicators (QI) are defined by National Institute for Health and Care Excellence as “measuring outcomes that reflect the quality of care or processes linked by evidence to improved outcomes”.
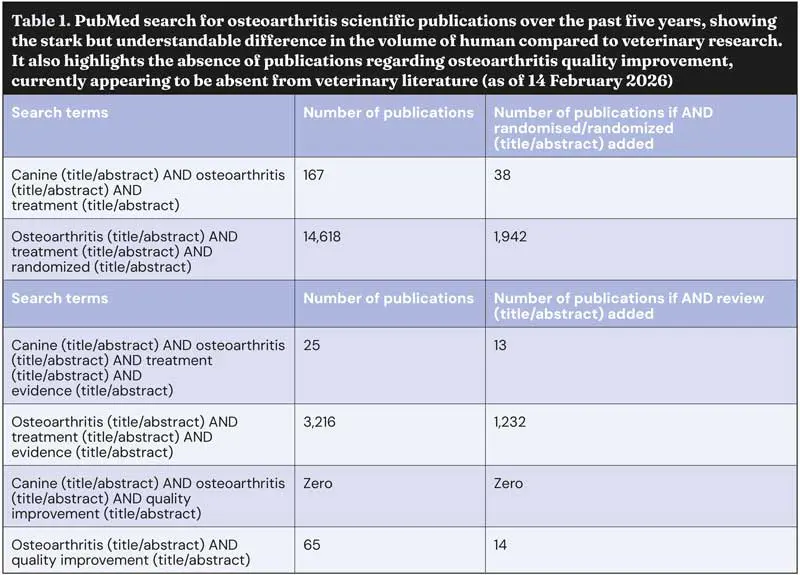
Understandable differences exist in the volume of veterinary compared to human OA research published over the past five years, but a stark difference also exists in any mention of quality improvement or QI (Table 1).
In human OA, the need to develop QI approaches to OA management has been honest and frank: “Due to a deficiency in clinical evidence, the quality of care was poor and inconsistent with many patients going undiagnosed and untreated” (Clohisy et al, 2024).
It is this honesty that has led human clinicians to define what effective care is and seek to measure this, review it and improve it: “[There] is no therapy that slows the disease progression of osteoarthritis. The main goal of management is to improve the quality of life by multimodal means, with non-pharmacological strategies focusing on modifiable risk factors as well as maintaining function and pharmacological strategies focusing on alleviating pain” (Duvnjak and Ammori, 2022).
In both prior mentioned studies, the authors sought to improve their management of individual OA patients, but also improve two words we should not fear: efficiency and productivity.
Improving these will result in better patient care and more clinical success, with an additional benefit in financial management. It is entirely likely that in veterinary medicine, similar initiatives along with improved team OA management could achieve the “nirvana” of improved patient and client care, higher staff morale, and, the author would suggest, reduce client costs yet increase our bottom line.
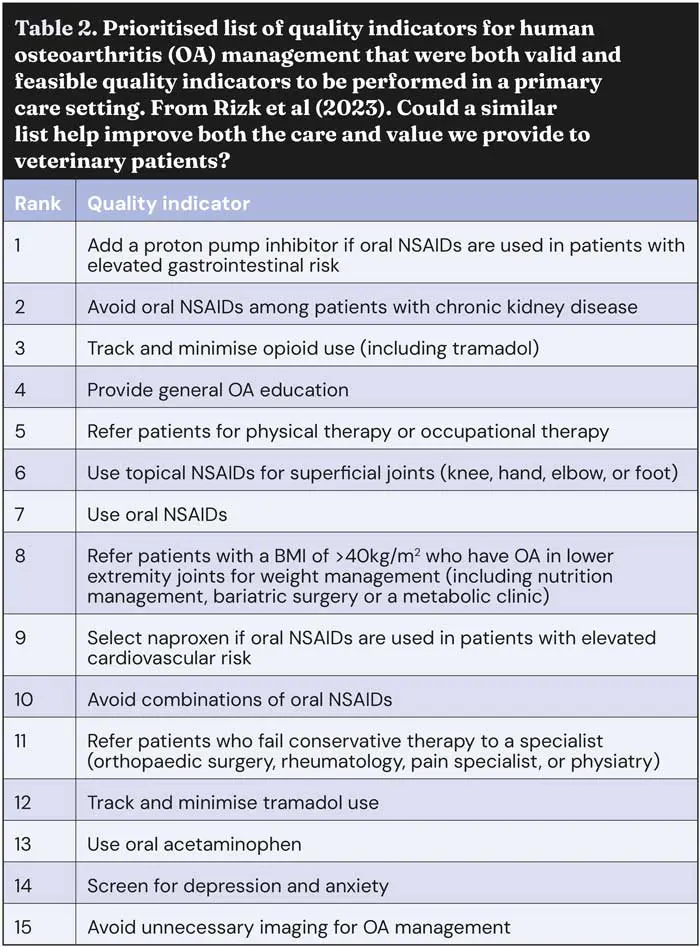
Some human research in this area is readily transferable to veterinary medicine. The paper, “Quality indicators for osteoarthritis pain management in the primary care setting” (Rizk et al, 2023), describes how the authors improved the adherence to guideline recommendations for OA, by developing a research programme embedded in a health system, established with buy-in from primary care and related specialists.
The objective of the project was to develop a set of consensus-driven, prioritised, valid and workable QIs that could be used to track quality initiatives for OA pain management in the primary care setting. These QIs were considered to be meaningful and relevant among stakeholders, not focusing on cutting edge, novel or bespoke therapies (Rizk et al, 2023).
The team deciding the QIs was predominantly composed of those responsible for delivery of care in the primary care setting. They started with more than 700 recommendations for OA management extracted from 41 published guidelines and, through assessing for validity and – most importantly – to ensure buy-in from primary care, the panel considered factors feasible within primary care. The result was 15 prioritised, valid and feasible QIs that can be used to track quality initiatives for OA pain management in the primary care setting (Table 2).
In a separate study, a local physiotherapy team described how they improved the management of knee pain OA from a level they felt to be “inconsistent” by introducing an exercise programme. This improved patients’ functional and strength-related outcome measures in those with knee OA; the programme was underpinned by Standards for Quality Improvement Reporting Excellence guidelines (Creasey et al, 2023).
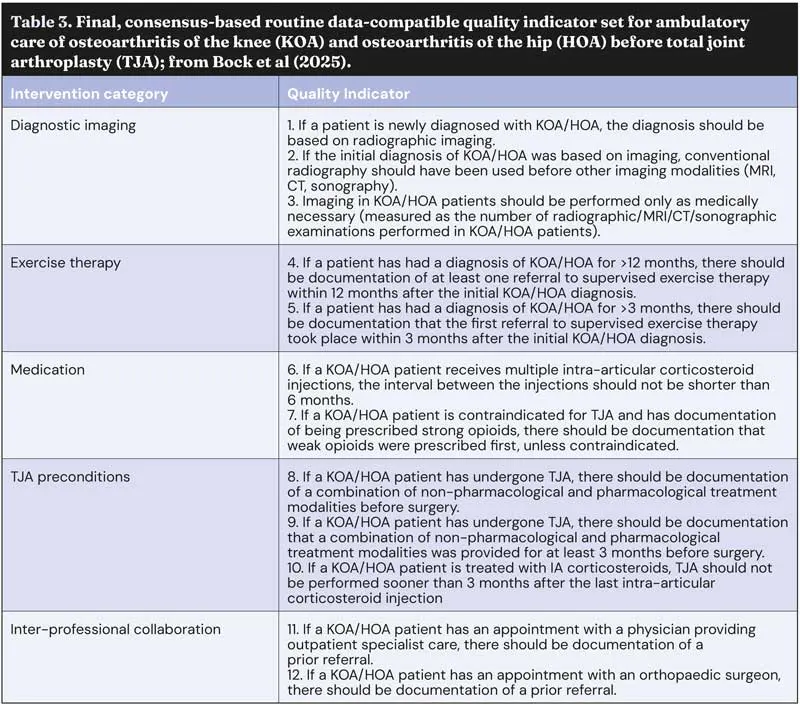
Another means of defining QI OA management aims was published by Bock et al (2025), who used the Delphi consensus process to define routine data-compatible QI for patients with knee and hip OA.
This technique resulted in a list of clearly defined QIs intended to support health care providers in monitoring and improving care processes, serving as a basis for identifying and addressing variation in care quality (Table 3).
One veterinary initiative already underway that seeks to change how we judge and influence success is the RCVS Knowledge Cruciate Registry.
The most recent 2025 report described ways in which participation in the project has increased vets’ confidence in treatment approaches and how they have been inspired to make changes, notably including reducing antibiotic prescribing.
Having clear, practice-specific information allows clinicians to have more open and informed discussions with owners about their pets’ expected recovery, likely function, and possible complications (RCVS Knowledge, 2025).
This project, which enables individual clinicians to review their personal clinical and customer satisfaction results relative to overall submissions, is an excellent example of how “real-world” data can directly impact on improving care more rapidly and locally than traditional research studies.
The factors surrounding veterinary care and OA management are complex, including patient needs, client desires, clinical limitations, finances, regulation, pharmaceuticals, and commercial aims.
The veterinary professions all share a desire to maintain – indeed, increase – our credibility to the public. By collaborating, being open and visible, and publishing our reasoning, we would strengthen the evidence behind our clinical decision making, enhancing our reputation.
Developing cross-sector research initiatives and publications in this arena would underpin our advice with our values: evidence, validity, feasibility and impact on outcome influencing clinical choices. This insight would be welcomed by many within primary care, not as a script, but as a platform to further support the provision of contextualised care within the wider reforms to emerge from the updated Veterinary Surgeons Act.
A further benefit of such initiatives would be a visible statement to the wider stakeholders about what the profession values – not to stifle innovation or development, but to more clearly outline what we want to improve, assisting those developing technologies and pharmaceuticals, for our patients.
Defining our own roadmap for improving the care we provide, for OA and other conditions, will empower all of us within the veterinary profession for years to come. Let’s do it – now.
Ross Allan graduated from the University of Glasgow in 2001, gaining his BSAVA Certificate in Small Animal Surgery in 2014 and RCVS Advanced Practitioner status in 2015. Ross is clinical director of referrals at Pets‘n’Vets, Glasgow where he leads Roundhouse Referrals, widening access to advanced veterinary surgery through innovative services such as “fixed-price” tibial plateau levelling osteotomy surgery. Working within the Roundhouse Veterinary Hospital, he is familiar with the challenges and reward in effectively supporting owners and treating pets with osteoarthritis.