19 May 2026
Gerry Henry BVMS, MRCVS looks at the health outcomes following surgery in this breed at eight weeks old.
Gerry Henry
Job Title
Image: Nynke / Adobe Stock
Surgical gonadectomy is still the principal means of controlling fertility in small companion animals. Numerous studies into the outcome of gonadectomy in dogs and cats have been conducted.
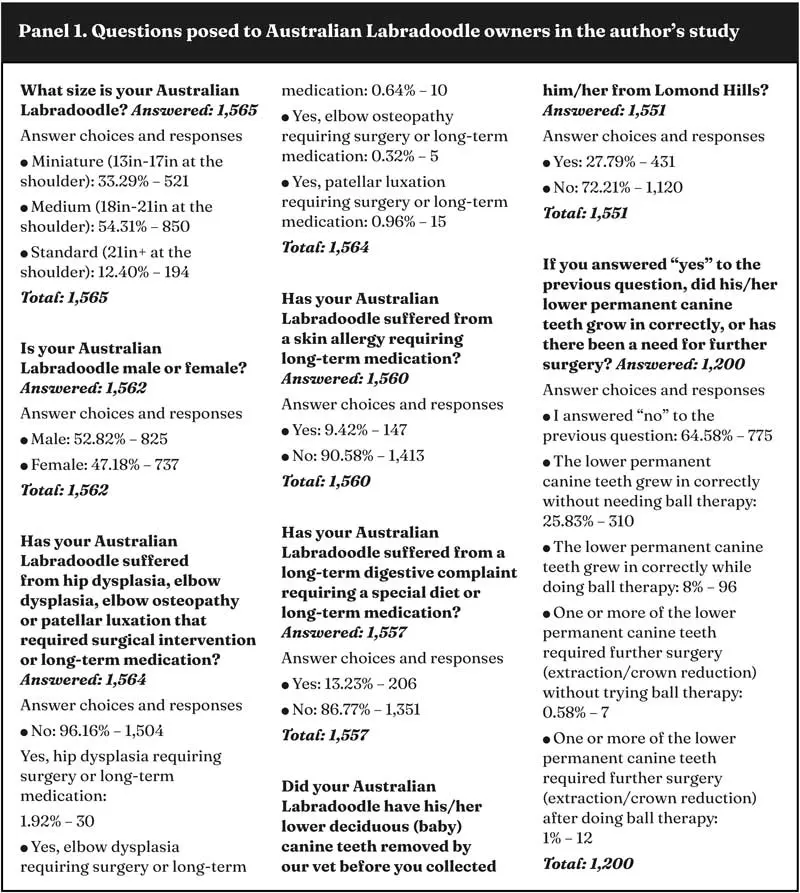
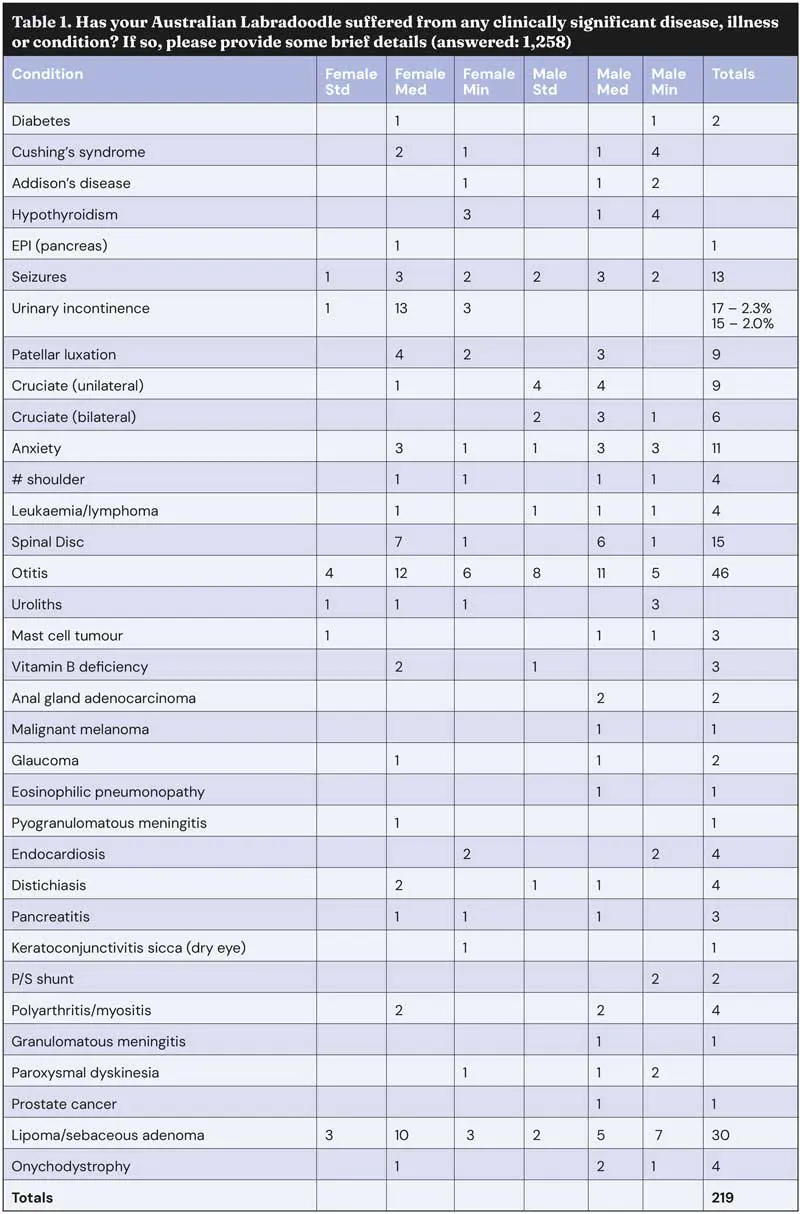
In 2024, these were collated by the WSAVA into a single review, the “WSAVA guidelines for the control of reproduction in dogs and cats”1. In the same year, the author conducted his own survey, which concentrated on the outcomes of prepubertal gonadectomy performed at eight weeks of age, in one breed (the Australian Labradoodle), in animals obtained from one breeder, by one veterinary surgeon, using the same anaesthetic protocol and surgical techniques. Just fewer than 2,000 emails were sent to persons who had purchased a puppy in the preceding 12 years; 1,565 replies were received. The questions and replies are presented in Panel 1 and Table 1.
All puppies to be operated on were eight weeks of age or slightly older. Weights varied but ranged between 2kg and 4kg, with an average of 2.8kg.
The puppies were premedicated with methadone (10mg/ml). Premedication at the lower dose of 0.05mg/kg was unsatisfactory and did not produce adequate analgesia. Puppies weighing between 2kg to 3kg were given a single injection of 0.20ml IM; puppies weighing between 3kg to 4kg were given a single injection of 0.22ml IM. Animals were premedicated 20 minutes before the procedure commenced, which gave good analgesia with minimal respiratory depression. A single injection of meloxicam (5mg/ml) was administered SC at the same time as the methadone.
General anaesthesia was induced using ketamine (100mg/ml) 0.05ml/kg bodyweight, and medetomidine 0.04ml/kg bodyweight, administered in the same 1ml syringe (three-part, low dead space, 25G × 5/8in needle) by IM injection into the lumbar muscles. Induction usually took around 60 seconds, during which time lubricating eye gel was applied to both eyes. Puppies were then intubated (cuffed endotracheal tube 3mm to 4.5mm, depending on size, connected to a T-piece) and maintained at 3L/sec oxygen with 0.5% isoflurane.
The area is clipped, prepped and draped. A midline incision is made through the skin and the linea alba, beginning from just below the umbilicus and extending caudally for 8mm.
The ventral mesentery may be partially removed at this stage if it appears sufficiently obtrusive to interfere with wound closure. A spay hook is introduced and run down the left lateral abdominal wall until it brushes the caudal pole of the left kidney. The ovarian ligament is then hooked and the left ovary gently exteriorised.
The suspensory ligament is identified and carefully released. This permits better access to the ovary and the vascular pedicle, which is then sealed and severed using bipolar forceps. The broad ligament is then broken down, freeing the ovary and proximal uterine horn.
The uterine body is located and, from there, the right uterine horn is tracked to the ovary. The process is repeated until the right uterine horn and ovary have been also freed. Both horns are amputated just above the uterine body using bipolar forceps. This is a subtotal ovario-hysterectomy; only the ovaries and uterine horns are removed. The uterus is handled carefully at all times, with minimal traction. The muscularis is closed with a single cruciate suture (4-0 USP). The subcutaneous layer is closed with a horizontal mattress suture (5-0 USP).
The skin is sealed with one or two drops of tissue glue, administered from a 1ml insulin syringe through a 30G needle (the animal is returning to a potentially contaminated environment, such as the puppy pen; also, the puppies are completely restored to normal activity within a few hours of surgery). Puppies are housed in heated pens on deep, soft, shredded paper. Faeces are regularly removed and although the recovery environment cannot be described as sterile, it is clean. The wound is not dressed.
Male puppies are anaesthetised in the same fashion. The scrotal area is clipped and prepped. A 5mm incision is made through the scrotal midline. The testicles are exteriorised (closed technique) and the cord is severed using bipolar forceps. The single skin incision is closed using one drop of tissue glue, as described previously.
Male puppies are Buster-collared for several days postop to prevent interference with the wound. Female puppies will normally ignore their wound. Animals are normally awake and extubated within 10 minutes of going into recovery. Puppies are bright, eating and playing with their litter mates within three hours.
Follow-up analgesia on the day after surgery is not deemed necessary. If the puppy has had deciduous canine teeth removed at the same time, oral meloxicam (1.5mg/ml) is given for a further three days. The incidence of skin dehiscence is less than 1%. No cases of complete wound breakdown have been recorded.
The most consistently discussed disadvantage of early gonadectomy in female dogs among the public and the profession is urinary sphincter mechanism incompetence (USMI). Although opinions on this matter are sincerely held, it must be acknowledged they are often based on outdated or incomplete information.
According to a study carried out in 2017, the incidence of urinary incontinence in adult female dogs following gonadectomy is between 3% to 20%2. The risk was reported to have increased if the procedure was performed between three and six months of age (such as before puberty)3.
However, in a review of the relevant literature published in the Journal of Small Animal Practice in 2012, only three studies were deemed to conform to the Cochrane guidelines, and the review concluded: “A systematic review of peer-reviewed original English analytic journal articles was conducted, based on Cochrane guidelines. Of 1,853 records screened, seven studies were identified that examined the effect of neutering or age at neutering on the risk of urinary incontinence but four were judged to be at high risk of bias.
“Of the remaining three studies, which were at moderate risk of bias, there was some weak evidence that neutering, particularly before the age of three months, increases the risk of urinary incontinence. However, overall the evidence is not consistent nor strong enough to make firm recommendations on the effect of neutering or age at neutering on the risk of urinary incontinence”4.
The published data – particularly if it disregards the effect of size and breed – can be confusing and seemingly contradictory. A case-controlled study in 2011 found no apparent correlation between the age of neutering and USMI5, while another reported gonadectomy between three and six months significantly increased the likelihood of female animals developing USMI in later life3. Current research suggests that breed, obesity and adult weight are more significant predictors of disease than the age at which the procedure was performed6.
In the author’s survey, only 2.3% of gonadectomised females (17 out of 737) were reported as affected by USMI in later life. If two dogs with contributing comorbidities are excluded, this drops to 2% (Panel 1).
The commonly accepted advantages of gonadectomy include the following.
Welfare. Reducing the number of uncared for animals in shelters or roaming free in our towns and cities; reducing the risks and stress associated with adult neutering.
Health. Reducing adverse health outcomes associated with intact reproductive organs. It is generally acknowledged that gonadectomised dogs live longer7.
A retrospective analysis of medical data from 2.2 million dogs revealed that gonadectomised female dogs lived on average 23% longer than intact female dogs8.
A perceived health benefit of early gonadectomy in female dogs is the “sparing” effect it has on mammary tumours (single and multiple, benign and malignant). The frequency of occurrence of mammary tumours in intact female dogs was described as ranging from 8.4% to 52%9. In gonadectomised females, it is generally accepted as being lower – as low as 1.8% in one study10.
Age at gonadectomy is important if the full sparing effect is to be achieved. In a study from 1969, the risk of mammary carcinoma was calculated as 0.5% in prepubertally gonadectomised females, 8% to 26% if gonadectomy was performed between the first and second cycle, or between the second and third cycle. No sparing effect was observed in female dogs spayed after the third cycle11.
In two more recent studies, no female dog that was gonadectomised before puberty was reported as developing a mammary tumour12,13. This is consonant with the author’s own study of 737 female Labradoodles aged between 6 months and 12 years of age, none of which (0%) have been reported as presenting with any type of mammary tumour.
The poodle “part” of the Labradoodle brought with it the predisposition to lingually displaced deciduous lower canines. Thanks to careful outbreeding, fewer affected animals are presenting than before, and the author is hopeful that, in the future, it will be greatly reduced, if not eliminated entirely. These figures are historic. The relatively high number of deciduous teeth removed is a reflection of seeing so many puppies under anaesthesia at the eight-week stage. The probability is many of these would have resolved in time without surgery and without leading to any abnormality of the permanent dentition. However, welfare considerations and a desire to achieve an optimal outcome favoured early intervention. The procedure (flap technique) is simple and straightforward, recovery is quick, and the outcomes, which include the following, are excellent.
Convenience. Reducing the problems associated with intact animals; oestrus bleeding and possible pregnancy in females; aggression, vagrancy, and hypersexuality in males.
Economic. Avoiding the expense of adult neutering and/or the expense of treating those diseases which affect or are caused by intact reproductive organs.
Proprietorial. Protecting blood lines and preventing unsuitable matings.
It could be argued that some of the most significant findings do not appear in the table since it is not possible to quantify a negative. In the female, no mammary tumours of any description; no cancerous or cystic ovaries; no diseases of the uterus including pyometra or cancer of the tubular tract; no vaginal tumours or prolapse.
In the male, no testicular tumours or torsion; no benign prostatic hyperplasia (or associated perineal hernia), no prostatitis; one case of prostatic cancer in an ageing (12-year-old) dog; no perianal gland tumours.
Gerry Henry qualified from the University of Glasgow in 1979 and was commissioned into the RAVC in the same year. He subsequently worked in the Ministry of Agriculture, Fisheries and Food during the worst of the BSE years before opening his own practices in Fife, Edinburgh and South Queensferry. He still practises part time in Fife and also in Great Yarmouth as a Greyhound Board for Great Britain-licensed veterinary surgeon.