3 Mar 2026
Kerry Brundell CertVNECC, RVN discusses what seizures are, what to do when a patient arrives and differentiating them from other syndromes.
Kerry Brundell
Job Title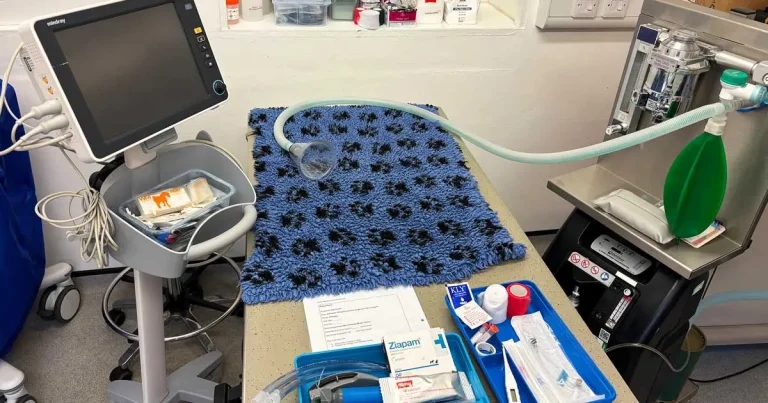
Figure 1. Equipment prepared for an emergency “seizuring” patient.
While it may seem obvious when a patient is having a tonic/clonic seizure, it is not always as easy to recognise, especially when a patient is having focal seizures. Other conditions have similar signs.
This article discusses the clinical signs of different types of seizures and compares these to other common conditions that may be mistaken for seizures. Careful questioning of the owner during history taking is fundamental to discerning a seizure from another disorder.
Triage, which is defined as the assessment of patients to determine the severity of their clinical signs and whether they need immediate treatment, is often first conducted over the phone (Covey, 2018).
It is difficult to make an accurate assumption based on the client’s opening words, as what they think to be a seizure could be another problem entirely. So, it is best to prepare for any scenario while awaiting the “seizuring” patient (Figure 1). However, as prolonged or recurrent seizures can cause irreversible cell damage, it is best to offer to see them as soon as possible to ensure treatments start swiftly (Hooper, 2021).
A seizure is a sudden, uncontrolled discharge of neurons in the cerebral cortex due to an imbalance of excitatory and inhibitory transmissions (Vite and Galban, 2018; Muńana, 2025).
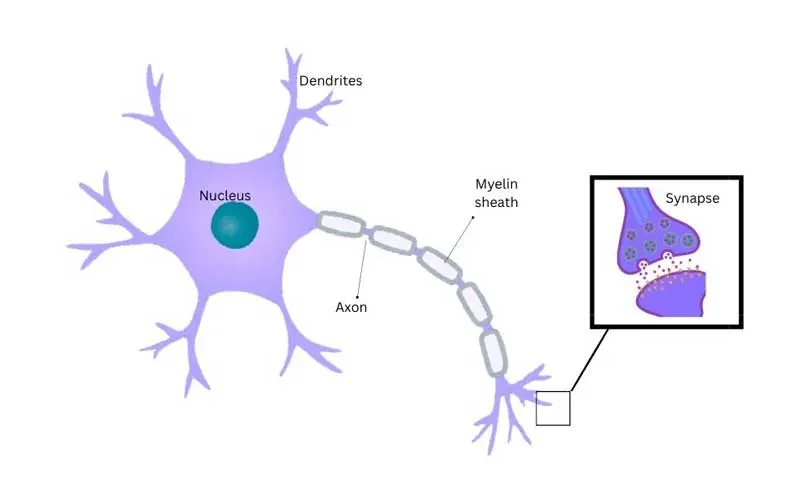
A neuron (Figure 2) is a cell that can communicate with another by creating an action potential that stimulates the release of neurotransmitters. These are released across a synapse to trigger another cell (Sanders, 2025a).
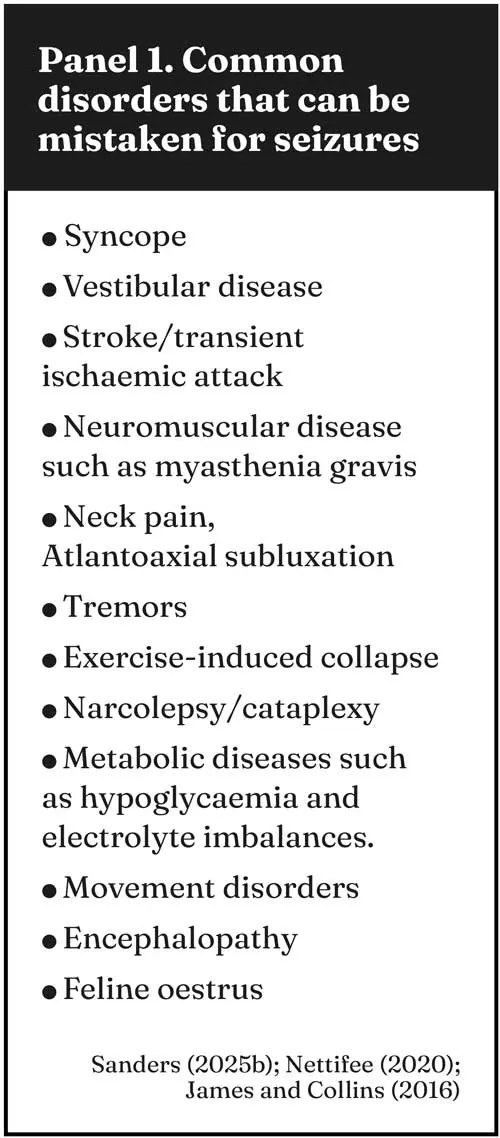
About 0.5% to 1% of the canine population present with seizures (Sanders, 2025a). This assumption that a pet has had a seizure based on the client’s view should always be investigated, as there are a great many other problems that may appear to be seizure-activity (Panel 1).
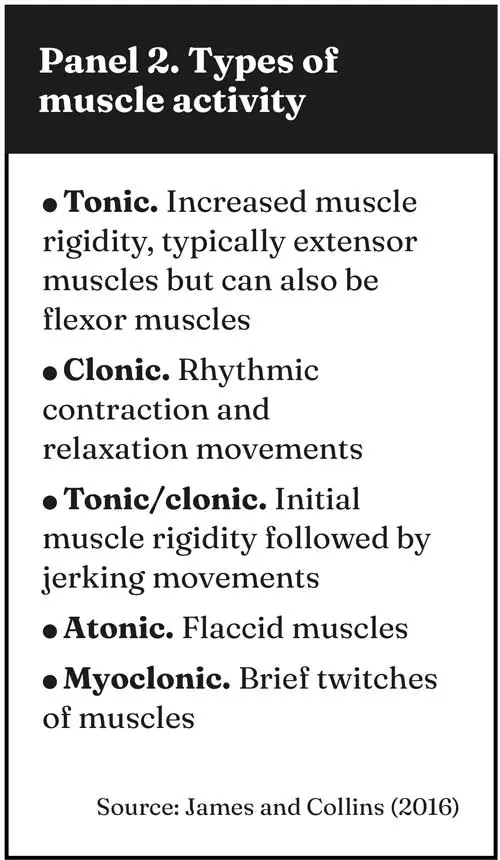
Seizures may present in different forms of muscular activity (Panel 2).
A generalised seizure occurs when both cerebral hemispheres are affected. Clinical signs include symmetrical tonic/clonic activity, myoclonus or atony (Vite and Galban, 2018).
A partial seizure occurs when only one region of the cerebral cortex is affected. This produces asymmetrical signs such as twitching on one side of the face, behaviour changes, tonus or clonus of one limb and turning the head to one side. The focal seizure activity can be found on the contralateral side to the area of the brain that is affected. Sometimes a partial seizure will progress to a generalised seizure (James and Collins, 2016).
A patient may be conscious during a partial seizure that makes it particularly difficult to diagnose if not witnessed. A definitive test for non-conclusive seizures is to perform an electroencephalogram (EEG), but this is not routinely done due to lack of access to equipment (Vite and Galban, 2018). A study by Granum et al (2019) found that 80% of the patients within their study showed no, or only subtle, signs of seizure activity, yet when an EEG was performed 21% of them were having seizure activity.
If time allows and it is safe to do so, owners can take video recordings of the seizure activity, which can aid veterinarians in diagnosis, yet Packer et al (2015) showed a low level of veterinarians in practice were able to interpret videos as seizure related or another paroxysmal event.
A primary assessment should be carried out, checking the major body systems (cardiovascular, respiratory and neurological) to determine any life-threatening conditions (Covey, 2018). A neurological system triage is based on checking their mentation, ambulation and presence of seizure activity (Brown and Drobatz, 2018).
If the patient is actively seizuring on arrival, this is deemed a category one and must be treated immediately (Covey, 2018). Flow-by oxygen may be necessary, as seizure activity increases the body’s oxygen consumption. Intravenous access can be challenging in a seizuring patient, so rectal or nasal anticonvulsants can be used.
Active cooling may also be needed, as hyperthermia is common following a period of seizure activity (Hooper, 2021).
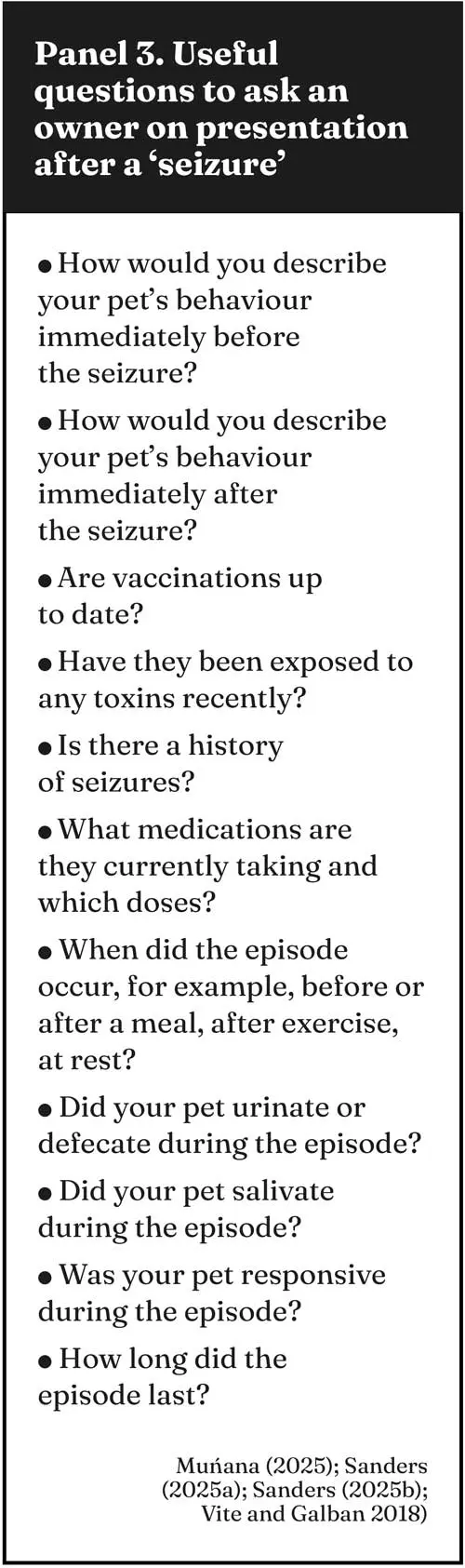
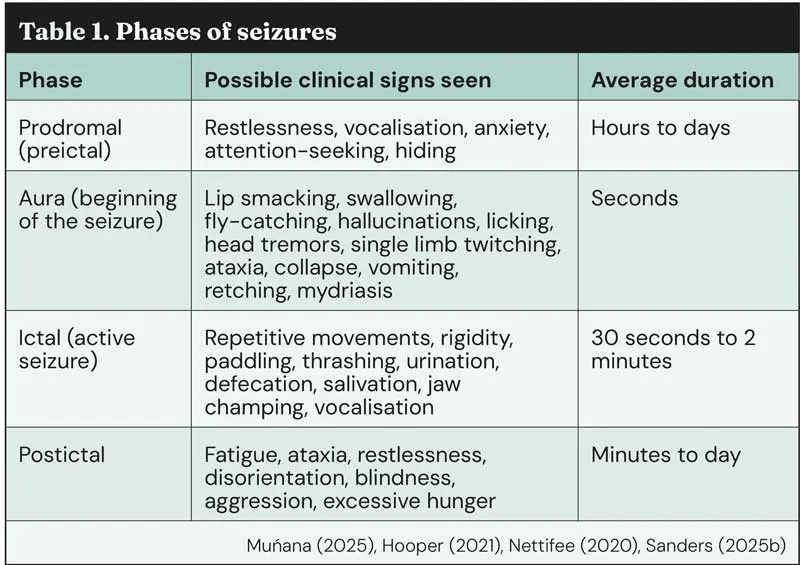
It is very important to question the owner closely to determine whether a seizure has occurred because, unless the patient is presenting in status epilepticus, the seizure has usually already passed. Panel 3 lists some helpful questions to ask the owners. Clinical signs of a seizure include behavioural changes before and after the seizure, involuntary motor activity, impaired consciousness, mydriasis, urination and defecation. The many clinical signs can be divided up based on the phase of the seizure (Table 1).
Seizures can be caused by head trauma, encephalitis, brain tumours, hypercalcaemia, hypernatraemia, hyponatraemia, hypoglycaemia, heat stroke, hepatic encephalopathy, toxicities, and thiamine deficiency. Many breeds are also predisposed to idiopathic epilepsy, including border collies, Belgium shepherds, beagles, Dalmatians, English springer spaniels, Labrador retrievers and Keeshonds (Vite and Galban, 2018; Figure 3).

Seizures are a symptom of a dysfunction of the brain and, as such, the cause must be investigated. It is prudent to take full bloods for haematology, biochemistry and electrolytes to aid in the diagnosis, but also be aware that seizure activity causes hypoglycaemia, hypoxia, acidosis and hyperlactaemia (Hooper, 2021). Total calcium, which is commonly reported by in-house laboratory analysers, measures ionised calcium as well as calcium bound to protein and anions. It is worth measuring only the ionised calcium, as this is the biologically active part that is responsible for clinical signs (Boag, 2018).
Further diagnostics are not always required if history and clinical signs suggest idiopathic epilepsy. However, advanced imaging, such as magnetic resonance imaging (MRI) and computed tomography (CT), are useful to detect any structural issues with the brain that could be causing seizures (Hooper, 2021).
Any space-occupying lesion within the brain can raise the intracranial pressure (ICP). This may lead to cerebral hypoxia, herniation and death, so these patients should be watched closely for signs of mental deterioration using the Modified Glasgow Coma Scale and for evidence of the Cushing reflex (bradycardia partnered with high blood pressure).
To ease the pressure within the brain, no jugular blood samples should be taken, no tight collars or leads should be placed around the neck, and the head should be raised to an angle of 15º to 30º (Hooper, 2021). Treatments such as mannitol or hypertonic saline may be prescribed by the veterinary surgeon. These should be followed with isotonic fluid therapy to prevent dehydration (Platt and Olby, 2013).
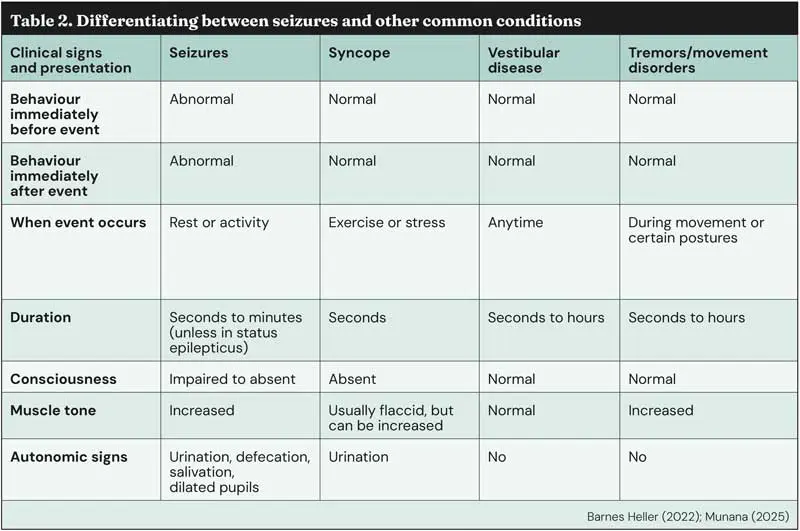
So, your patient arrives at the practice and careful questioning of the owner and examination of the patient has revealed seizure activity probably hasn’t occurred. What else could it be? Table 2 outlines the main differentials with their presenting signs and history.
The vestibular system is responsible for maintaining balance and orientation. The sensory receptors for this are located in the semi-circular canals of the inner ear (Muńana, 2013). These patients are often presented as emergencies, as the clinical signs can be distressing for both the patient and the owner (James and Collins, 2016).

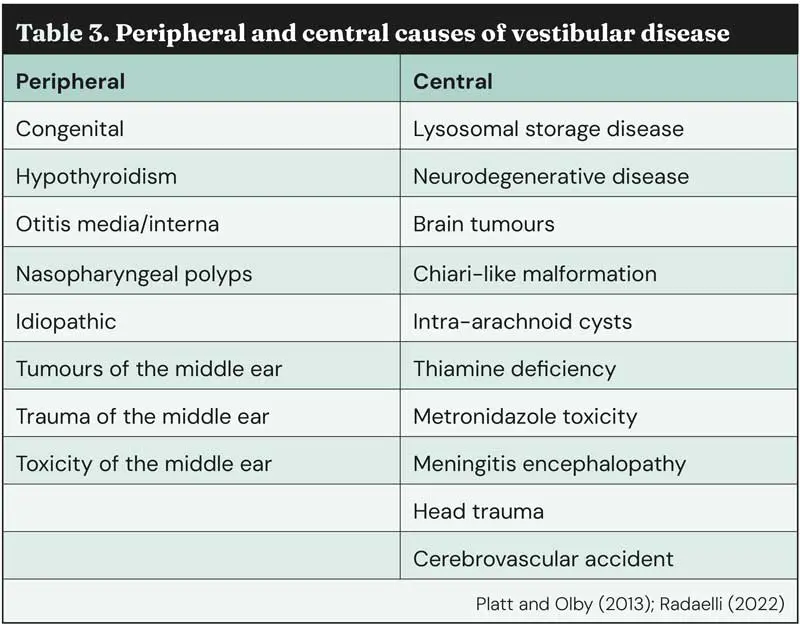
Vestibular disease should be localised to a central or peripheral cause (Table 3).
If neuro-localisation reveals a central problem, further diagnostics should include MRI or CT to assess for structural abnormality of the brain (Figure 4). This is important to do before any cerebrospinal fluid (CSF) is sampled, as this may be dangerous if there is any increase in intracranial pressure (Radaelli, 2022).
While not strictly a neurological disease, syncope is very often confused by owners as a seizure.
Syncope is a sudden loss of consciousness due to a decrease in cerebral perfusion with a spontaneous recovery. Factors that may cause this include a raised ICP, reduced cardiac output and reduced vascular resistance (Charalambous et al, 2017).
Barnes Heller (2022) and Muńana (2025) note the comparisons in clinical signs of syncope and seizures (Table 2). While some similarities exist between these two conditions, such as loss of consciousness and urination, many more differences can be seen, so questioning the owner is invaluable to diagnosis. However, a mild syncopal episode may not produce a total loss of consciousness, but only hindlimb ataxia, and a severe episode may induce brief tonic spasms due to hypoxia making it look much more like a seizure (Charalambous, 2017).
Tremors are involuntary, rhythmic movements, which make it difficult for the patient to stand and ambulate. There are no autonomic signs displayed and the clinical signs may last for hours (Gandini, 2024). Tremors can be classified by their type (Liatus and De Decker, 2023):
Tremors can be breed-related, for example, Scottie cramp in Scottish terriers, and episodic falling syndrome in cavalier King Charles spaniels. Other breeds predisposed to movement disorders are English bulldogs, Norwich terriers, Border terriers and soft-coated wheaten terriers (Gandini, 2024).
Tremors may also manifest after ingestion of tremorgenic toxins such as mycotoxins, pyrethrins, metaldehyde, caffeine, xylitol, permethrin and cannabis (Liatus and De Decker, 2023).
It is important to question the owner on ingestion of any potential toxins so that treatments can be tailored to a particular toxin, such as intralipid therapy (Figure 5).
The only definitive way to differentiate between focal seizures and tremors is to perform an EEG (Gandini, 2024), but as these are not readily available see Table 2 for characteristic signs of each condition.
Animals with neck pain may present as emergencies at the practice with or without accompanying neurological deficits. Signs of neck pain include depression, vocalisation, ventroflexion of the neck, stiffness, spasms of the neck, reluctance to move, salivation, dilated pupils and increased heart and respiratory rates (Platt and Freeman, 2013).
Neck pain can be caused by cervical disc herniation, atlantoaxial instability, syringomyelia with Chiari-like malformation and meningoencephalitis, especially steroid-responsive meningitis-arteritis (Olby, 2013).
Neck spasms (myoclonus) are a common finding in animals with neck pain. A 2025 study by Martinez et al showed that intervertebral disc disease was the most common form of non-epileptic myoclonus in various dog breeds.
Chiari-like malformation is a reduced volume in the caudal fossa due to congenital hypoplasia, which causes the cerebellum to herniate through the foramen magnum. This affects the outflow of CSF to produce a pocket within the parenchyma of the spinal cord known as syringomyelia (Platt and Freeman, 2013).
This is often seen in small and toy breed dogs, notably the CKCS. The presenting clinical signs are neck pain, phantom scratching, vocalisation and even tetraparesis (Platt and Freeman, 2013).
In summary, with many differentials in the “seizuring” emergency, history taking and a thorough examination, together with diagnostics, are imperative to making a diagnosis and starting the correct treatment.
Kerry Brundell works at an independent veterinary practice where she is a multi-disciplinary nurse, having previously worked at two large referral centres in the UK. She qualified as an RVN in 2008, gained her CertVNECC in 2021 and is working towards the ISFM certificate in feline nursing. She lives in Suffolk with her family, her Labrador and her cat.