26 May 2026
Luca Ferasin DVM, PhD, CertVC, PGCert(HE), DipECVIM-CA(Cardiology), GPCert(B&PS), FRCVS and Heidi Ferasin BVSc, CertVC, MRCVS argue the case for these “forgotten” and “essential” tools to be used more on a day-to-day basis.

Image: New Africa / Adobe Stock
Electrocardiography (ECG) has been part of veterinary medicine for more than half a century, yet its role in general practice has never been fully realised.
While echocardiography, radiography and laboratory diagnostics have become routine, ECG has gradually slipped into the background. Many clinicians rely heavily on auscultation and structural imaging, forgetting that disturbances in cardiac electrical activity are often invisible without rhythm assessment.
Holter monitoring, despite being the gold standard for detecting intermittent arrhythmias, is even less frequently used, and is often reserved for referral settings or specialist centres.
This diagnostic gap has real consequences. Dogs and cats with syncope, collapse and falling events, episodic weakness, or exercise intolerance frequently undergo neurological investigations, behavioural assessments or empirical therapy before anyone considers the heart as a possible aetiology. Many arrhythmias are intermittent, stress or exercise dependent, or nocturnal and may, therefore, be missed on a standard five-minute ECG. Without rhythm monitoring, clinicians may overlook life-threatening conditions such as paroxysmal atrioventricular block, supraventricular tachycardia or ventricular tachycardia. In cats, the problem is even more pronounced, as syncope is often misinterpreted as seizure activity, leading to unnecessary anticonvulsant therapy and delayed cardiological assessment.
The purpose of this article is to re-establish ECG and Holter monitoring as essential components of small animal practice. It will explore why these tools have been forgotten, how their underuse affects patient outcomes and practice revenue, and how modern telecardiology services now make rhythm diagnostics accessible to every clinician. Recent evidence, including a study on pre-anaesthetic ECG screening published in the Veterinary Record (2024), will be integrated to highlight the contemporary relevance of these tools.
The decline of ECG in general practice is not due to lack of utility; rather, it reflects a combination of misconceptions, practical barriers, equipment availability and shifting diagnostic habits. Furthermore, many clinicians feel under-confident interpreting ECGs, believing that only cardiologists can accurately diagnose arrhythmias. The waveform terminology, lead configurations and arrhythmia patterns can appear daunting – especially without regular exposure. This leads to a misconception that ECG interpretation is the exclusive domain of specialists. In reality, recording an ECG is simple, and interpretation can be outsourced to telecardiology services, if needed. The barrier is often not the test itself, but the fear of misinterpretation.
Another factor contributing to ECG’s decline is the over-reliance on echocardiography. However, while echocardiography detects structural and functional abnormalities, it does not uncover electrical instability. A normal echocardiogram does not rule out arrhythmias. In fact, many of the most dangerous arrhythmias occur in patients with structurally normal hearts. In one of the authors’ feline Holter studies, 8 of 13 cats had unremarkable resting ECGs, yet all 13 displayed arrhythmias on Holter monitoring. This single observation illustrates the limitations of relying solely on resting ECG or echocardiography.
Underestimation of arrhythmias as a cause of clinical signs also contributes to the problem. Syncope, episodic weakness and exercise intolerance are frequently misattributed to neurological or behavioural causes. Without ECG or Holter monitoring, arrhythmias remain undiagnosed, sometimes until the patient experiences sudden death. Cats are particularly prone to misdiagnosis. In a review of feline syncope, it was noted that many cats experiencing syncope are misdiagnosed with epilepsy and undergo expensive, and often unnecessary, diagnostic investigations.
Practical barriers also play a role. Many practices still rely on old ECG units with poor signal quality, dried electrodes or cumbersome paper print-outs. Others have no ECG or Holter equipment at all, or rely solely on instantaneous multi-parameter monitoring devices. However, free-loan equipment models, such as those offered by some telecardiology providers, eliminate this barrier entirely, providing modern, high-quality devices without capital expenditure.
Finally, a persistent perception exists that ECG and Holter monitoring are time consuming. In reality, a standard ECG takes less than 3 minutes to record, and a Holter takes just 5 to 10 minutes to fit. These are among the most efficient diagnostics available. Furthermore, to mitigate frequent time constraints within a busy clinical setting, ECG recording and Holter attachment can readily be performed by qualified veterinary nurses, whose involvement not only streamlines workflow but also strengthens their sense of clinical contribution. Many nurses report feeling more valued and engaged when entrusted with these procedures, and their participation naturally enhances their skills and confidence in cardiac monitoring.

The underuse of ECG and Holter monitoring has significant clinical implications. Many arrhythmias are intermittent and, therefore, missed on a resting ECG. Without Holter monitoring, clinicians may miss paroxysmal supraventricular tachycardia, intermittent atrioventricular block, ventricular tachycardia, sinus node dysfunction, or bradyarrhythmias frequently associated with syncope. These conditions can cause exercise intolerance, falling and fainting (syncope), or even sudden death.
Syncope is often misinterpreted as epilepsy – especially in cats. Without ECG or Holter monitoring, clinicians may pursue neurological investigations, behavioural assessments or empirical anticonvulsant therapy. This delays appropriate treatment and increases costs for pet owners. In dogs, syncope associated with intermittent atrioventricular block or ventricular tachycardia may be overlooked until the arrhythmia becomes sustained or the patient experiences a life-threatening event.
Anaesthetic risk is another important consideration. Undiagnosed arrhythmias increase the risk of peri-anaesthetic complications. Bradyarrhythmias, conduction disturbances and ventricular ectopy can all complicate induction and maintenance of anaesthesia. The Veterinary Record (2024) study demonstrated that even in clinically healthy dogs, pre-anaesthetic ECG can reveal abnormalities that influence anaesthetic decision making. This study provides contemporary evidence supporting the value of ECG in routine pre-anaesthetic assessment.
Delayed cardiology referral is another consequence of underusing ECG and Holter monitoring. Without rhythm assessment, clinicians may overlook early signs of cardiomyopathy or conduction disturbances. Early detection allows for timely referral, appropriate therapy and improved outcomes. In breeds predisposed to arrhythmogenic cardiomyopathy, such as the boxer, Dobermann, great Dane, German shepherd dog, mastiff and so on, Holter monitoring is essential for early detection and risk stratification. Similarly, in some larger canine breeds, the first indication of a severe underlying atrioventricular valve anomaly may be the development of an arrhythmia, even when a murmur is not readily appreciable.
The clinical implications of underusing ECG and Holter monitoring extend far beyond the immediate risk of missing an arrhythmia; they influence the entire diagnostic pathway, often diverting clinicians towards investigations that are more expensive, more invasive or simply less relevant. A dog with episodic collapse may undergo neurological imaging, blood tests and empirical anticonvulsant therapy before anyone considers the possibility of an intermittent arrhythmia. A cat with sudden weakness or transient disorientation may be labelled epileptic, anxious or geriatric, when in fact the underlying problem is a transient conduction disturbance.
These misdirections are not the result of negligence, but of habit; a habit formed in an era when ECG was perceived as a specialist tool rather than a routine diagnostic test.
The intermittent nature of many arrhythmias compounds the problem. A five-minute ECG is a snapshot, not a film. It captures a moment in time, and that moment may be entirely normal even in a patient with significant cardiac electrical disturbances. This is particularly true for paroxysmal arrhythmias, which may occur only during excitement, exercise, sleep or stress. A dog with paroxysmal atrioventricular block may have a perfectly normal ECG in the consulting room, only to collapse hours later at home. A cat with intermittent ventricular tachycardia may show no abnormalities during a brief recording, yet experience dangerous arrhythmias during the night. Without Holter monitoring, these events remain invisible.
The consequences of missing these arrhythmias can be profound. Syncope is not a benign event. It reflects a transient loss of cerebral perfusion and, while the episode itself may be brief, the underlying cause may be life threatening. Ventricular tachycardia, high-grade atrioventricular block and sinus node dysfunction can all lead to sudden death if left untreated. Even less dramatic arrhythmias can have significant consequences. Persistent tachyarrhythmias may lead to tachycardia-induced cardiomyopathy, a reversible but potentially severe form of myocardial dysfunction. Bradyarrhythmias may cause exercise intolerance, lethargy or collapse, reducing quality of life and increasing risk during anaesthesia.
Anaesthesia represents a particularly vulnerable moment for patients with undiagnosed arrhythmias. Many anaesthetic agents depress myocardial function, alter autonomic tone or influence conduction pathways. A dog with an unrecognised atrioventricular block may tolerate everyday activity without incident, yet develop profound bradycardia under anaesthesia. A cat with intermittent ventricular ectopy may experience exacerbation during induction or recovery. The study published in the Veterinary Record (2024) underscores this point, demonstrating that even clinically healthy dogs, animals with no murmurs, no clinical signs and no known cardiac disease, may harbour ECG abnormalities significant enough to influence anaesthetic planning. Without routine ECG screening, these abnormalities remain undetected, and anaesthetic risk increases unnecessarily.
The diagnostic consequences extend beyond anaesthesia. Many systemic diseases influence cardiac rhythm, including hyperthyroidism, hypothyroidism, electrolyte disturbances, gastrointestinal disease and other abdominal pathologies. A cat with hyperthyroidism may develop supraventricular tachycardia or atrial premature complexes. A dog with Addison’s disease may show bradyarrhythmias or conduction disturbances. Without ECG, these manifestations may be missed, delaying diagnosis and treatment of the underlying condition.
The underuse of ECG also affects the management of known cardiac disease. Dogs with myxomatous mitral valve disease or atrioventricular valve dysplasia can frequently develop atrial fibrillation or ventricular ectopy as the disease progresses. Cats with hypertrophic cardiomyopathy may experience atrial premature complexes or ventricular tachycardia. Without ECG monitoring, these developments may go unnoticed, leading to suboptimal therapy and increased risk of decompensation. Holter monitoring is particularly valuable in these patients, providing detailed information about arrhythmia burden, circadian variation and response to therapy.
The clinical consequences of underusing ECG and Holter monitoring are compelling enough on their own, but the financial implications for general practice are equally significant.
ECG and Holter services represent a substantial revenue opportunity, yet many practices fail to capitalise on them. This is not due to lack of demand or utility, but to lack of awareness. The cases are already in the building: geriatric patients presenting for routine health checks, animals undergoing dental procedures or lump removals, dogs with occasional collapse or falling episodes, cats with vague episodes of weakness, patients with known cardiac disease requiring assessment or monitoring, and pedigree breeds with predisposition to arrhythmogenic cardiac disease requiring health screening. Each of these cases represents an opportunity to provide valuable diagnostic information while generating revenue for the practice.
The economics are straightforward. ECG requires minimal time, minimal equipment and minimal consumables. The procedure can be performed by a trained nurse in minutes, freeing the veterinarian to continue with their tasks. Holter monitoring requires slightly more time to fit the device, but once applied, it generates no additional workload until the recording is complete. Interpretation can be outsourced to telecardiology services, eliminating the need for in-house expertise. The practice charges for the procedure, the interpretation and the report, generating income with minimal overheads.
Despite this, many practices perform only a handful of ECGs each month and even fewer Holters. This represents a missed opportunity not only for revenue, but for improved patient care. Practices that integrate ECG and Holter monitoring into their routine workflows often find that these services become a natural part of their diagnostic repertoire. Pre-anaesthetic ECG becomes standard for geriatric patients. Holter monitoring becomes routine for dogs with intermittent collapse or breeds predisposed to cardiomyopathy.
Over time, these services become embedded in the culture of the practice, benefiting patients, clients and clinicians alike.
The financial benefits extend beyond the direct revenue generated by ECG and Holter services. Early detection of arrhythmias leads to earlier intervention, which in turn leads to improved outcomes. Clients appreciate proactive care and are more likely to trust and return to a practice that identifies problems early.
Practices that offer comprehensive cardiac assessment differentiate themselves from competitors, attracting clients who value thoroughness and expertise. Telecardiology services further enhance this value by providing specialist interpretation, ensuring that reports are accurate, detailed and clinically actionable.
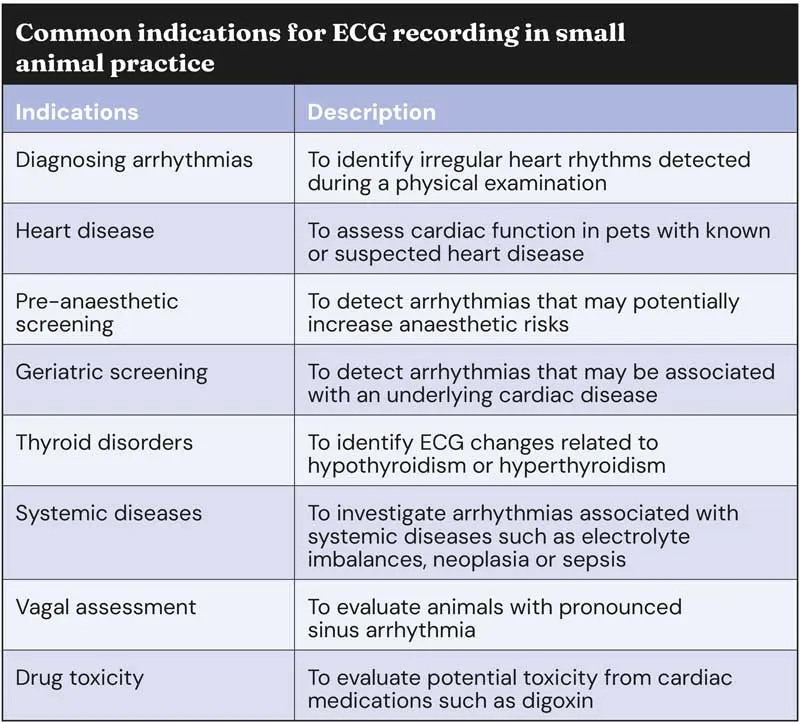
ECG remains the gold standard for diagnosing arrhythmias and conduction disturbances. Its value lies not only in its diagnostic specificity, but in its immediacy. An ECG provides real-time information about the electrical activity of the heart, revealing abnormalities that may not be apparent on physical examination or imaging.
In general practice, ECG is particularly valuable in patients presenting with syncope, collapse, episodic weakness or exercise intolerance. It is also essential in the assessment of tachycardia, bradycardia, irregular rhythms and suspected drug toxicity.
The utility of ECG extends beyond the identification of arrhythmias. It provides insight into conduction intervals, waveform morphology and chamber enlargement; for example, prolonged PR intervals may indicate first-degree atrioventricular block. Wide QRS complexes may suggest bundle branch block or ventricular origin. Tall R waves may reflect left ventricular enlargement, while deep S waves may indicate right ventricular enlargement. ST segment changes may suggest myocardial hypoxia or electrolyte disturbances. These findings, while not definitive on their own, contribute to a broader understanding of the patient’s cardiac status.
ECG is particularly valuable in pre-anaesthetic assessment. Many arrhythmias are clinically silent and may only be detected during routine screening. Identifying these abnormalities before anaesthesia allows clinicians to modify protocols, avoid drugs that exacerbate bradycardia or conduction disturbances, and plan for intraoperative monitoring and support.
The Veterinary Record (2024) study reinforces this point, demonstrating that even clinically healthy dogs may harbour ECG abnormalities significant enough to influence anaesthetic planning.
In addition to its diagnostic value, ECG plays a crucial role in monitoring therapy. Patients receiving antiarrhythmic drugs require periodic ECG assessment to evaluate efficacy, optimise dosing and detect adverse effects. Digoxin, for example, can cause characteristic ST segment changes and arrhythmias that are readily identified on ECG. Beta blockers and calcium channel blockers may cause bradycardia or conduction disturbances.
Without ECG monitoring, these effects may go unnoticed, leading to suboptimal therapy or adverse outcomes.
ECG also provides valuable information in systemic diseases that influence cardiac rhythm, as previously outlined, allowing clinicians to identify these manifestations and tailor therapy accordingly.

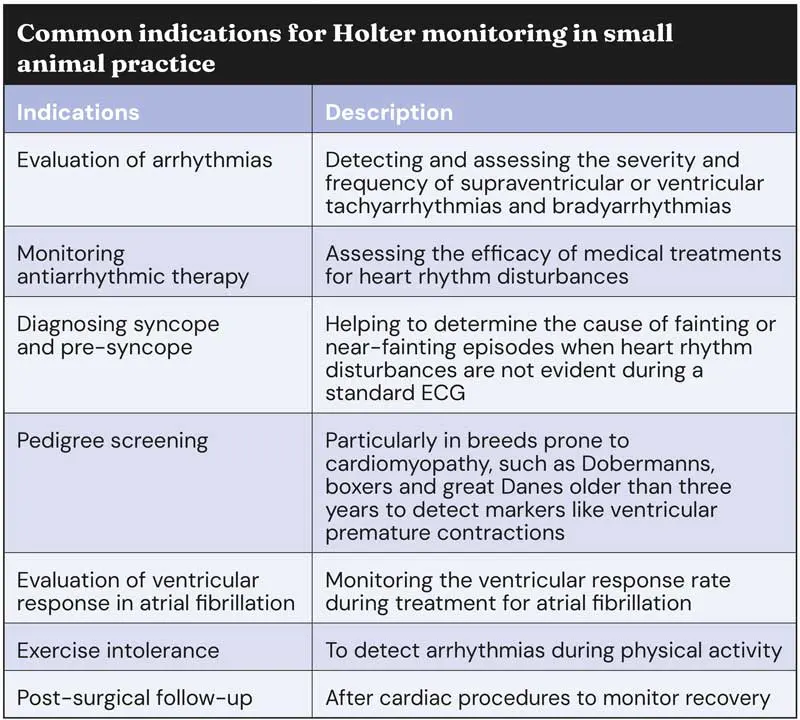
Holter monitoring occupies a unique and indispensable place in veterinary cardiology because it captures what a standard ECG cannot: the rhythm of the heart as it behaves during the patient’s normal life. While a resting ECG provides a snapshot, a Holter recording provides a narrative. It reveals the ebb and flow of autonomic tone, the influence of sleep and activity, the impact of stress, and the presence of arrhythmias that appear only fleetingly. For many patients, this difference is not merely academic; it is the difference between a missed diagnosis and a life-saving intervention.
The value of Holter monitoring becomes particularly clear when considering the nature of paroxysmal arrhythmias. These events may occur only a handful of times per day, or even per week, and may be triggered by excitement, exertion or sleep. A dog with paroxysmal atrioventricular block may experience long pauses only during periods of high vagal tone, such as at night or during rest. A cat with intermittent ventricular tachycardia may show no abnormalities during a brief ECG in the consulting room, yet experience dangerous arrhythmias during the early hours of the morning, for example. Without continuous monitoring, these events remain invisible, and the patient remains at risk.
Holter monitoring also provides invaluable information about arrhythmia burden. A dog with occasional ventricular premature complexes may have a benign condition, or it may have a high burden of ectopy that places it at risk of sudden death. A cardiopathic cat with occasional atrial premature complexes may be stable, or it may be on the cusp of developing atrial fibrillation. The number, frequency and pattern of arrhythmias matter, and only Holter monitoring can provide this level of detail. This information guides therapy, informs prognosis and shapes decisions about referral, medication and monitoring.
In breeds predisposed to cardiomyopathy, Holter monitoring is not merely useful; it is essential. Boxers with arrhythmogenic right ventricular cardiomyopathy may show no structural abnormalities on echocardiography, yet have significant ventricular ectopy on Holter. Dobermanns with dilated cardiomyopathy (DCM) may have normal echocardiograms early in the disease (occult DCM), yet show ventricular arrhythmias long before structural changes become apparent. In these breeds, Holter monitoring is a screening tool, a diagnostic tool and a prognostic tool, all at once. It allows clinicians to identify disease early, initiate therapy promptly and monitor response over time.
Holter monitoring is equally valuable in feline cardiology. Cats are notoriously difficult to assess using resting ECG because they are often stressed in the clinic, and their arrhythmias may be subtle or intermittent. In the authors’ feline Holter study, all 13 cats displayed arrhythmias on Holter, despite eight having unremarkable resting ECGs. This finding underscores the limitations of relying solely on brief recordings in feline patients. Holter monitoring provides a window into the cat’s true cardiac rhythm, revealing arrhythmias that may be clinically significant even when the heart appears structurally normal.
Holter monitoring also plays a crucial role in the assessment of therapy. Antiarrhythmic drugs require careful monitoring to ensure efficacy and detect adverse effects. A dog receiving sotalol or mexiletine for ventricular tachycardia may show improvement on resting ECG, yet continue to experience significant arrhythmias during the night. A dog with atrial fibrillation may show an appropriate instantaneous heart rate in clinic, but an inappropriately fast average ventricular response rate when assessed over a 24-hour period. A cat receiving beta blockers may develop bradyarrhythmias that are not apparent during brief recordings. Holter monitoring allows clinicians to evaluate the true impact of therapy, adjust dosages, and ensure that treatment is both safe and effective.
Finally, Holter monitoring provides valuable information in the assessment of pacemaker function. Over-sensing, under-sensing and inappropriate pacing may not be apparent during brief ECG recordings. Holter monitoring allows clinicians to evaluate pacing percentage, detect abnormalities and ensure that the device is functioning correctly. This is particularly important in patients with complex arrhythmias, those who have undergone recent pacemaker implantation or in pacemaker patients displaying ongoing or recurrent clinical signs.
The study by Bustamante and colleagues (Veterinary Record, 2024) provides contemporary evidence supporting the value of routine ECG screening in general practice. The study evaluated 228 clinically healthy dogs undergoing elective procedures, all of which had normal physical examinations and no known cardiac disease. The aim was to determine whether routine pre-anaesthetic ECG screening influenced the decision to request echocardiography or modify anaesthetic protocols.
The findings were striking. Nearly one-third of dogs had ECG abnormalities, despite being clinically healthy. These abnormalities ranged from benign variations to findings significant enough to warrant further investigation. Echocardiography was recommended in a small subset of dogs, and all dogs that underwent echocardiography had structural abnormalities. This suggests that ECG screening not only identifies electrical abnormalities but may also reveal underlying structural disease that would otherwise remain undetected.
Perhaps, most importantly, anaesthetic protocols were modified in more than 15% of dogs with ECG abnormalities. These modifications included changes in premedication, induction agents and intraoperative monitoring. In some cases, the presence of arrhythmias prompted clinicians to avoid drugs that exacerbate bradycardia or conduction disturbances. In others, the findings led to increased vigilance during anaesthesia, with adjustments to monitoring and support. Without ECG screening, these abnormalities would have gone unnoticed, and anaesthetic risk would have increased unnecessarily. The authors of the study concluded that routine pre-anaesthetic ECG screening was useful for promoting echocardiography and influencing anaesthesia plans in a subset of dogs. This conclusion reinforces the value of ECG in general practice and highlights the importance of specialist interpretation. Many ECG abnormalities are benign, while others require further investigation or protocol modification. Telecardiology services provide the expertise needed to distinguish between these categories, ensuring that clinicians receive accurate, actionable information.
The implications of this study extend beyond anaesthesia. They highlight the broader value of ECG as a screening tool in general practice. Many dogs and cats appear clinically healthy yet harbour electrical abnormalities that may influence their long-term health. Routine ECG screening allows clinicians to identify these abnormalities early, initiate appropriate monitoring, and provide proactive care. This approach aligns with the broader trend in veterinary medicine toward preventive care and early intervention.

Telecardiology has transformed the accessibility of ECG and Holter interpretation in general practice. Services such as www.ecg4vets.com provide specialist interpretation within hours, detailed reports with clinical recommendations, and free-loan ECG and Holter equipment. This model eliminates the two main barriers to ECG use: lack of confidence in interpretation and lack of modern equipment.
General practitioners can now record ECGs and Holters with confidence, knowing that a cardiologist will provide accurate, actionable interpretation. Telecardiology also improves patient outcomes by enabling early detection of arrhythmias, timely referral and appropriate therapy. It enhances practice revenue by making ECG and Holter services accessible and profitable. The integration of telecardiology into everyday workflows represents a significant step forward in the delivery of cardiac care in general practice.
Telecardiology also supports continuing education. Clinicians receive detailed reports that explain findings, provide context and offer recommendations. Over time, this exposure enhances clinicians’ understanding of ECG interpretation and arrhythmia management. It fosters a culture of learning and collaboration, benefiting both clinicians and patients.
Introducing ECG and Holter services into general practice requires minimal investment. Staff can be trained to record ECGs in minutes, and telecardiology services provide interpretation. ECG can be offered as part of pre‑anaesthetic assessment, geriatric or pedigree screening, or investigation of clinical signs such as syncope, collapse, or exercise intolerance. Holter monitoring can be scheduled for patients with intermittent signs, breeds predisposed to cardiomyopathy, or those receiving antiarrhythmic therapy.
Client communication is essential. Owners should be informed that ECG is quick, painless and inexpensive, and that Holter monitoring provides valuable information about their pet’s heart rhythm. Early detection of arrhythmias improves outcomes and reduces the risk of sudden death. Practices that communicate the value of these services effectively often find that clients are receptive and appreciative.
When using telecardiology services, pricing should reflect the diagnostic value and cost of specialist interpretation. Practices should consider offering ECG as part of pre-anaesthetic packages or geriatric health checks. Holter monitoring can be offered as a premium service for patients with intermittent signs or those requiring long-term monitoring. Over time, these services become a natural part of the practice’s diagnostic repertoire, benefiting all.
When resting ECG is normal but clinical signs persist, Holter monitoring should be considered. If Holter monitoring is inconclusive and syncope is infrequent, an implantable loop recorder may be appropriate. These devices provide long-term rhythm monitoring and can capture arrhythmias that occur only a few times per year. They represent the next step in the evolution of rhythm diagnostics and are increasingly accessible in veterinary medicine.
ECG and Holter monitoring are indispensable tools in modern veterinary cardiology. Their underuse in general practice represents a missed opportunity, both clinically and financially.
By rediscovering these “forgotten essentials”, clinicians can dramatically improve diagnostic accuracy, enhance patient outcomes and strengthen practice revenue.
Telecardiology services remove all barriers, providing specialist interpretation and free-loan equipment that make ECG and Holter monitoring accessible to every practice, every day. The message is simple: if you are not routinely recording ECGs and Holters, your patients and your practice are missing out.
Use of some of the drugs in this article is under the veterinary medicine cascade.
Luca Ferasin is the director of Specialist Veterinary Cardiology Consultancy, which has provided cardiac services in the UK for more than 10 years. With more than 30 years of clinical, academic and telemedicine experience, Luca founded ecg4vets as a modern, accessible telecardiology service for veterinary practices. Today, he continues to lead the clinical direction of ecg4vets while serving as co‑director of Hampshire Veterinary Cardiology. He is a regular speaker worldwide and his main professional interests include feline cardiology and exercise physiology, as well as investigation and management of syncope and coughing.
Heidi Ferasin graduated from the University of Bristol in 2005. Heidi is an experienced cardiologist and has been an RCVS advanced practitioner in veterinary cardiology since 2015, having held the RCVS Certificate in Veterinary Cardiology since 2010. Heidi is co-director of Specialist Veterinary Cardiology Consultancy and Hampshire Veterinary Cardiology. She is also a co-founder of ecg4vets, a veterinary telecardiology service specialising in ECG and Holter services. Heidi has participated in many international research projects relating to both canine and feline cardiology, with numerous publications in these fields and is a regular invited speaker, both within the UK and internationally. Heidi is actively involved in the teaching and mentoring of post-graduate veterinary surgeons and veterinary nurses.