9 Jun 2026
Ed Cooper BVSc, MRCVS and Allie Matchwick BVSc, BSc(Hons), MANZCVS(Small Animal Surgery), CertAVP, DipECVS, MRCVS explore how this is possible and how it helps to reduce antimicrobial resistance.
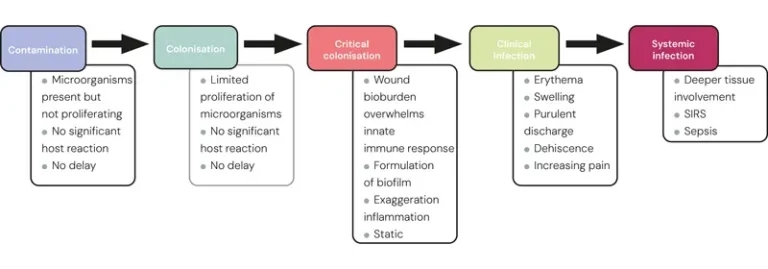
Figure 1. Sequential effects of increasing bacterial numbers and virulence in a wound.
Wounds in companion animals are difficult to study in a controlled manner due to the wide spectrum of presentations and the ethical difficulties in creating experimental wounds with controls. For this reason, it is often necessary to extrapolate human or equine evidence when trying to improve our practice.
A role may exist for creating working groups, where practitioners can share their knowledge and experience to widen our knowledge base, in absence of reliable clinical data.
Antimicrobial resistance (AMR) is becoming an increasing problem for the human and veterinary fields, and has been shown to be directly correlated to increasing antimicrobial (AM) use.
It is estimated that in the coming decades, the number of human deaths attributed to AMR will rise steeply, with a review in 2016 estimating up to 10 million deaths annually by 2050 (O’Neill, 2016).
It is possible we may see this trend reflected in veterinary medicine. As vets, we have a responsibility to both our patients and their owners to try to combat this problem. With a plateau in the discovery of new AM and potential restrictions for veterinary use, prudent choices have never been more important.
Nolff et al (2016) demonstrated a strong positive correlation between wounds treated with prior AM and the culture of multidrug-resistant (MDR) bacteria. Furthermore, several studies have highlighted the potential inefficacy of systemic AM for wounds: no reliable reduction of bacteria in granulation tissue (Robson et al, 1974); low AM concentration in interstitial wound fluid (Polykandriotis et al, 2019); and a limited effect in the presence of a biofilm.
All wounds contain bacteria, and it is important that we correctly diagnose clinically relevant infection. Figure 1 demonstrates the sequential effects of increasing bacterial numbers and virulence in a wound.
As wound healing still progresses despite contamination or colonisation, the aim is not to create a wound free of bacteria. Wounds in these stages do not require treatment, and wounds that are critically colonised require topical treatment only.
Clinically infected wounds may need to be treated with systemic AM; however, many can be effectively treated with topical therapy and AM dressings alone. Wounds with concurrent systemic signs (SIRS/sepsis) do require systemic AM treatment.
It is vital that if systemic AM are used, use is based on bacteriology results, with cytology to guide initial treatment. However, a positive culture in the early stages of wound contamination/colonisation is not an indication to start therapy in the absence of clinical signs of infection (Lipsky et al, 2016).
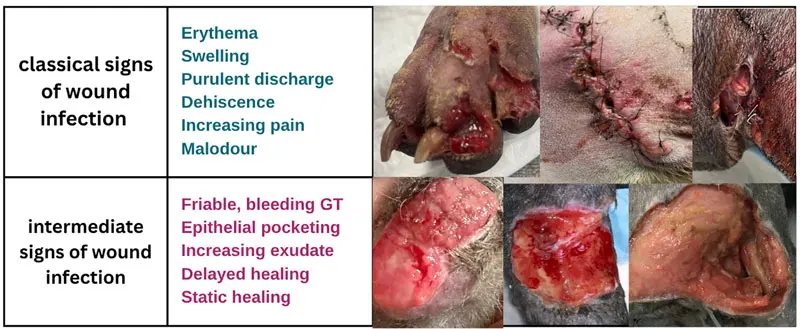
It is, therefore, crucial we can recognise the signs of a clinically infected wound. Clinical wound infection can present with “classic” or “overt” clinical signs, or more subtle “intermediate” or ‘”overt” symptoms (International Wound Infection Institute, 2022; Figure 2).
Biofilms form when free-floating bacteria attach to a surface, such as necrotic tissue or an implant, and secrete a protective extracellular matrix protecting the bacteria. More free-floating bacteria are shed, attaching to other areas of the wound bed. The immune response produces exudate that further protects and nourishes the biofilm.
Bacteria within biofilms can grow at a slower metabolic rate with fewer nutrients and less oxygen, cultures can be negative, and cells can become up to 1,000 times less susceptible to antimicrobial agents.
Biofilms should be suspected in chronic non-healing wounds, infections recurring after cessation of AM, wounds with implants or sequestrae, and areas with reduced vascularity. Mechanical disruption is the only effective treatment for biofilms.
As previously outlined, wounds with signs of systemic infection will require AM cover. Other indications for systemic AM treatment of a clinically infected wound include:
Cytology and culture and sensitivity should be performed – ideally with a tissue sample rather than a surface swab – and while pending culture results, broad-spectrum AM such as potentiated amoxicillin or cefuroxime/cefalexin should be commenced.
In cases with rods on cytology, or cases that have had a prior AM course and a wound infection where a treatment delay could adversely affect outcome, a fluoroquinolone could be added in the first instance and de-escalated as appropriate (BSAVA, 2024).
When selecting an appropriate AM, consider the likely organisms involved such as Enterococcus species, Escherichia coli, Pseudomonas species and Pasteurella species (Nolff et al, 2016). Using an appropriate AM dose, route and frequency is essential to reduce the risk of AMR development. Fixed AM courses are increasingly debated; treatment should be guided by clinical resolution (Sousa et al, 2022).
Systemic AM are not indicated for wounds consistent with a cat bite abscess without pyrexia or cellulitis; acute superficial traumatic wounds, snake bites, superficial localised bite wounds without pyrexia or cutaneous dehiscence of a surgical site without evidence of clinical infection or pyrexia (BSAVA, 2024).
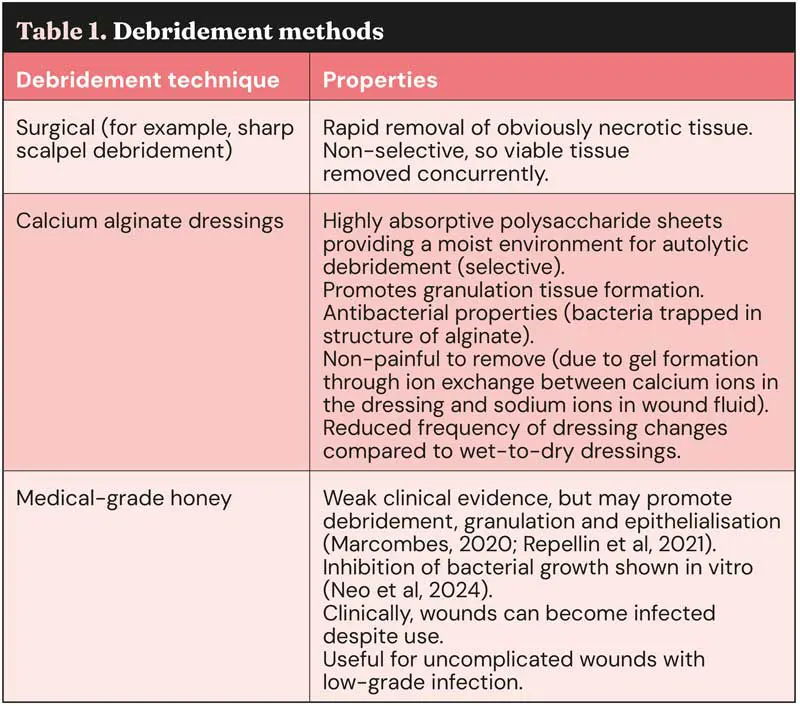
Necrotic tissue or foreign material must be removed from wounds, as it will prolong the inflammatory phase and promote biofilm formation. Debridement can be split into selective and non-selective methods (Table 1).
Wet-to-dry dressings have been historically used during the inflammatory phase and often seem to be very effective; however, their use is now contraindicated (non-selective debridement, pain on dressing removal requiring sedation and maceration of the wound edge) and we have better alternatives.
Hydrocolloid and hypertonic dressings are available, and have debriding properties, but compared to alginates these both have disadvantages. Hydrocolloids are excessively occlusive, and hypertonic dressings are often painful on application.
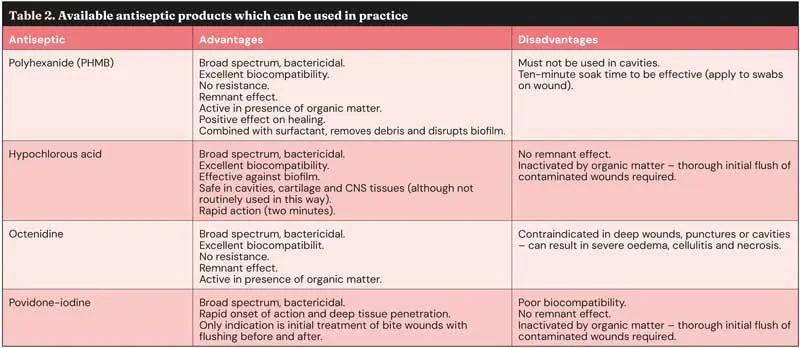
Antiseptics are an essential component for treating clinically infected wounds. The ideal antiseptic treatment is:
Table 2 shows some examples of available products that can be used in practice.
Chlorhexidine, while still the standard of care for surgical site preparation, is contraindicated in wounds. This is largely due to its narrow safety window for cytotoxicity and increasing resistance levels.
Topical antibiotics are typically not advised for use in wounds due to promotion of resistance and potential cytotoxic effects (Lipsky et al, 2016). AM dressings are an excellent alternative.
An ideal AM dressing would have the following characteristics:
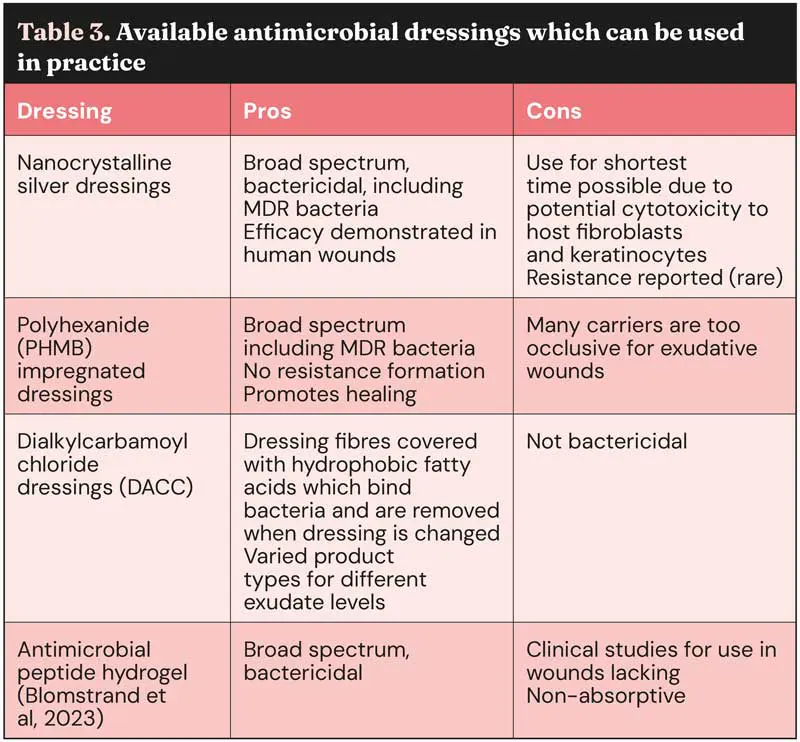
The carrier of the AM agent (for example, polyurethane foam versus alginate versus hydrocolloid) needs to be carefully chosen depending on the moisture level of the wound; for example, Acticoat (Smith and Nephew) is a silver-based dressing, but has no absorptive properties, so is not suitable for exudative wounds.
Table 3 shows some examples of available products that can be used in practice.
Negative pressure wound therapy (NPWT) is becoming increasingly available in veterinary settings. This is an excellent option for managing clinically infected wounds and provides an optimum wound environment, namely a moist wound without fluid accumulation, encouragement of perfusion and reduction of bacterial proliferation. Silver dressings and antiseptic instillation can be incorporated for AM purposes. A recent meta-analysis in people has found superior wound healing when NPWT is combined with alginate dressings (He and Yang, 2026).
A photo should be taken of every wound at every visit to allow monitoring and assessment of progress by different clinicians. These should be added to the patient record or an easily accessible, centralised, online location; for example, a Microsoft Teams channel. An increased range or change in the stock of wound products should be combined with educational initiatives for clinical staff.
Clinical audit has been shown to be highly effective as part of AM stewardship strategies and can be performed in practice to monitor AM use for wounds. The findings should be reported back to clinical staff and discussed. Days of AM treatment per wounded patient can be used to indicate prescribing trends for wounds, the overall pressure for AMR and the increasing use of alternative wound treatments.
It is possible to treat clinically infected wounds without using systemic antibiotics.
This should reduce the development of AMR bacteria within the wound and the environment, which benefits the patient, the owner, clinical staff, and society.
Ed Cooper graduated from the University of Bristol’s Veterinary School in 2019 and subsequently worked in charity practice in the UK and Australia for several years before taking an ECC role in Melbourne. More recently, he has completed a rotating internship at a referral centre in the south-west of England and is currently working in small animal practice in Gloucestershire.
Allie Matchwick graduated from the University of Bristol in 2012 and worked in small animal general practice for five years before focusing on surgery. She completed her residency in private practice and became an ECVS/EBVS boarded specialist in small animal surgery in 2024. Allie currently works at Eastcott Referrals, doing both soft tissue and orthopaedic cases, with a mostly orthopaedic bias. She has interests in wound management, antimicrobial stewardship for wounds and the treatment of open fractures. Allie is also secretary of the Veterinary Wound Healing Association.