2 Dec 2025
Nicola Robinson BSc, MA, VetMB, MRCVS considers how professionals can help owners to prevent potential poisonings, and explains why it is crucial to treat the patient, not the poison.
Nicola Robinson
Job Title
Lilium species.
This article will provide guidance on what vets should be aware of before poisoning cases present, so that they are ready to tackle them to the best of their abilities.
This will ensure that patients receive the most appropriate treatments, common pitfalls are avoided and there is the highest chance of a successful outcome – both in terms of the pet’s health and the owner’s perception about how the case was handled.
Carrying out a risk assessment on each individual case is essential before treatment starts to decide whether it is needed.
If the patient is asymptomatic or only showing mild signs, there is time to do this, and it is important to not have a blanket protocol for all animals presenting with poisoning. The key is not to start treatment until you know that it is indicated – particularly in cases where the effects from the toxin are likely to be milder than the treatment you are planning, which may be invasive and unpleasant for the patient.
The risk assessment involves working out exactly what the animal has been exposed to and by which route. The active ingredient needs to be established, as well as the strength (if applicable) and amount. This involves careful questioning of the owner and asking them to bring in any packaging, if possible. Sometimes, the active ingredient is not an issue, but an excipient is toxic, so looking at the full ingredient list of a product is important.
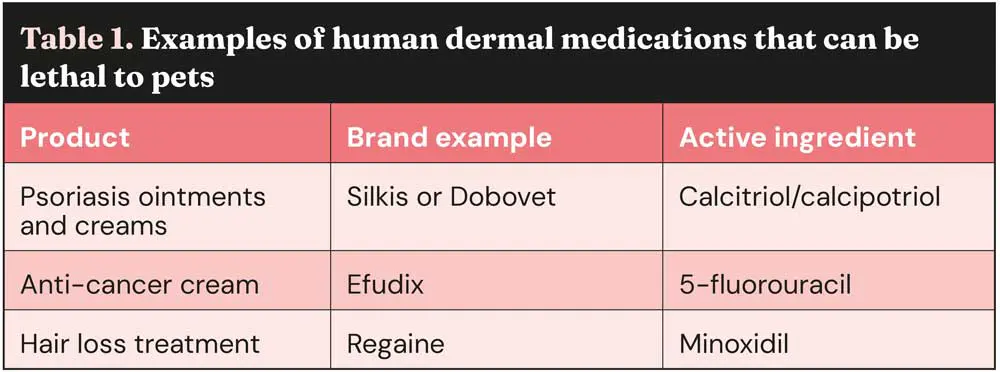
Quantity alone is not always an indicator to treat – it is the toxic dose that is important. There are some medications where a significant number of tablets can be ingested with little effect and no treatment is needed, while others are extremely toxic at very low doses. Some dermal medications are particularly toxic and can cause serious clinical signs or fatalities at very low doses; for examples, see Table 1.
Vets often know how to treat the common toxins, but treatment plans should be tailored to the individual case – so, remember to treat the patient, not the poison.
It is important to have a specific plan in place for the patient, taking into consideration all the necessary factors. Treatment protocols will vary in complexity depending on the species of animal affected (some toxins affect species differently; for example, xylitol in dogs or Lilium species in cats), route of exposure, amount/dose, patient’s weight, time after exposure, clinical signs and any pre-existing conditions.
Time since exposure is particularly important, since toxins are absorbed at different rates. Inducing emesis after one hour is too late for some agents (such as salt, xylitol and naproxen) and, therefore, not worthwhile. However, some substances remain in the gut for a prolonged period, such as raisins and sultanas; therefore, later emesis may be worthwhile.

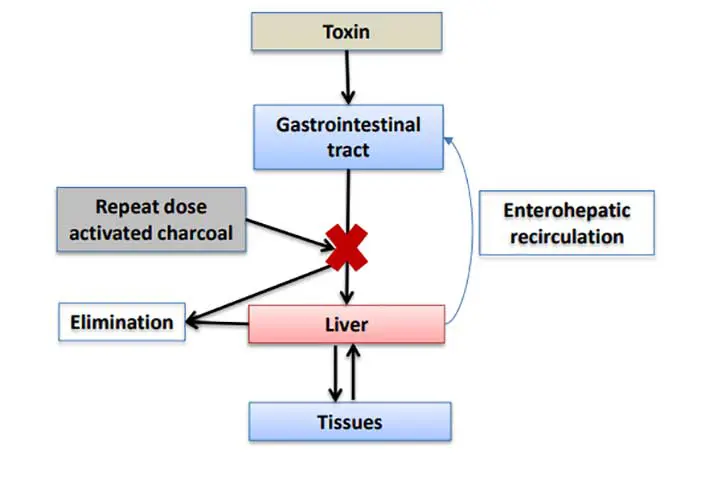
A single dose of activated charcoal is appropriate for most poisoning cases, but the charcoal needs to be in contact with the ingested substance, and so should be given as soon after ingestion as possible. For toxins that undergo enterohepatic recirculation, the window for repeated doses of activated charcoal is longer (approximately 24 hours), but if this has passed, then it is not worth giving any because it will be ineffective. There are other cases when emesis should definitely not be induced.
A few examples of these include:
Initial thoughts about a toxic exposure may not be correct; for example, thinking that if a dog has eaten rat poison, it must be an anticoagulant and it needs gut decontamination and vitamin K, when there are actually eight different anticoagulants, each with its own toxic dose, so treatment may not be required, even with large ingestions. Added to this, there are other types of rodenticides to consider, notably vitamin D, which can cause hypercalcaemia and, if not treated appropriately from the start, irreversible calcification of the tissues.
The treatment plan would, therefore, be completely different from an anticoagulant rodenticide.
Treatment plans can vary from giving one dose of activated charcoal in some cases, to long periods of intensive nursing and monitoring for others. The latter may mean that referral to an OOH provider is required, with financial implications for the owner.
Consulting a veterinary poison centre in these instances can help tailor the plan according to the progression of the signs and the individual circumstances of the owner, advising what the impact on the prognosis is depending on which route is taken.
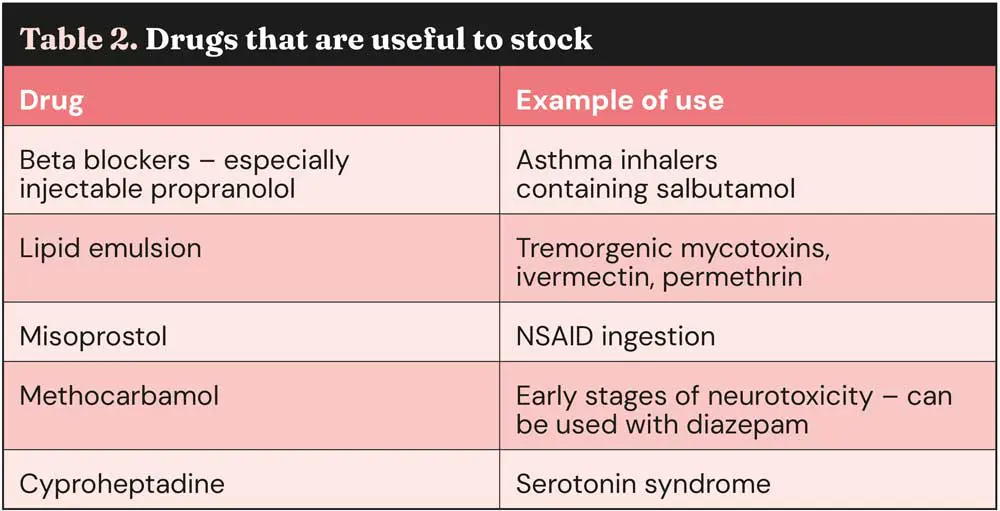
Some medications are very useful in poisoning cases and are regularly recommended, but they are often not in stock (Table 2).
Many owners do not appreciate that toxicology is a specialist area of veterinary medicine and often think that vets should know how to treat all poisons without understanding the need for external support.
The World Health Organization (WHO) states that “poison centres are sources of specialised expertise to address the fact that health professionals could not be expected to know about the toxicity of every chemical substance and product, and also to provide a focus for toxicological research” (WHO, 2020). This is equally true for veterinary and human poison centres.
In addition to providing advice on case management, poison centres play a crucial role in toxicovigilance and research. They continuously collect and analyse case data and trends, identify new risks, and gather information on the toxicology of pharmaceuticals and other agents, including any new products that come to the market.
Case follow-up information is essential for refining treatment advice and understanding toxic doses, onset, duration of clinical signs, and outcomes. Vets are encouraged to report poisoning cases to poison centres to contribute to this data collection. A case or two involving a specific substance in a single veterinary hospital may not raise suspicion, but several cases reported to a poison centre may act as a signal for a larger issue.
There are very few specific veterinary poisons centres in the world, located in the UK, France, US and Australia. The Veterinary Poisons Information Service (VPIS) was launched in 1992, amassing almost 400,000 cases on its database since then and handling more than 25,000 cases per year.
Many online sources contain misleading, conflicting, wrong, potentially dangerous or outdated treatment recommendations and advice on poisoning. Poison centres are a specialist resource for vets and pet owners, providing accurate, up to date and tailored advice.
In the UK, there are two services for poisoning advice: Animal PoisonLine (APL) for owners and the VPIS for veterinary professionals.
It is worth noting that they are completely different services, and it is important to know how they differ to select the right one at the time of a poisoning case.
For information including fees and contact details, visit the APL (www.animalpoisonline.co.uk) and VPIS (www.vpisglobal.com) websites. Approximately 80 per cent of owners do not need a vet visit after an APL consultation. If an owner does need to go in for treatment, the vet can call the VPIS using their membership for full treatment advice tailored to the individual case, if required. In these cases, the owner is refunded the APL fee.
On the APL line, we do not go through treatment with the owner, since it would not be safe or appropriate to expect them to relay this to the veterinary practice. However, if they need a vet visit, we do inform them why immediate treatment is needed, how serious the case is and try to manage their expectations regarding what will happen at the vets (such as level of treatment); for example, we may say that hospitalisation is or is not required, or that it is too late to make their pet sick, but that there is another treatment to absorb the toxin that the vet can give.
If an owner informs the practice of this advice and the vet wants to just confirm that this is in fact what was discussed, they can call the VPIS line for free. A credit is only charged when full management advice is given, including expected signs, timescales, treatment and prognosis.
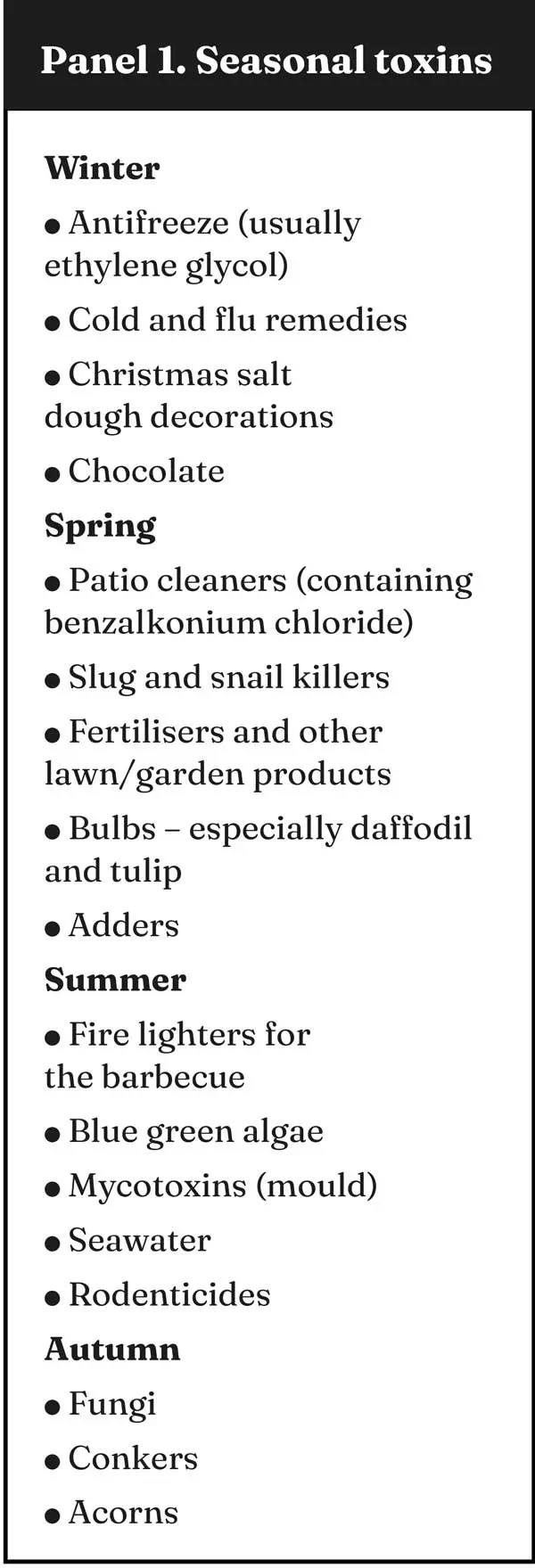
It is worth knowing which toxins you are likely to see at different times of the year so that they are top of your list if a patient comes in with specific signs but no witnessed ingestion. See Panel 1 for some common poisons by season.
However, the most common agent group the VPIS are called about is drugs, which is not seasonal. The group includes both human and veterinary pharmaceuticals (the most common being ibuprofen, paracetamol and meloxicam), as well as drugs of abuse (mainly cannabis). They represent around 40 per cent of the total call volume.
Owners are usually very worried when they think their pet has been poisoned and have nearly always consulted Google before contacting their vet, which does not help. Giving consistent advice is key.
We all want the pet to receive the right treatment from the start, so working together to ensure that we all give the same clear advice will lead to owners feeling reassured about the process.


The APL and VPIS lines are open 24 hours a day, all year round, so we are here if a veterinary professional or owner needs us. All our calls are recorded, and we are liable for the information we give you, so we hope our service will help reduce the stress that these cases can cause.
We support veterinary professionals throughout the course of their poisoning case, so that we can work together to get optimal clinical outcomes whenever possible.
Nicola Robinson BSc, MA, VetMB, MRCVS, studied zoology at the University of Bristol, followed by veterinary science at the University of Cambridge, and worked as a vet in companion animal and equine practice for 16 years. In 2015, she joined the Veterinary Poisons Information Service (VPIS), answering poisons enquiries from vets, and in 2016 was promoted to her current role as head of service. In 2017, Nicola launched Animal PoisonLine, the 24-hour advice line for pet owners run by the VPIS.
