13 May 2013
Kevin Eatwell suggests medical options for treating otitis before advising on optimum surgical techniques, precautions and prognosis for rabbit patients.
Kevin Eatwell
Job Title
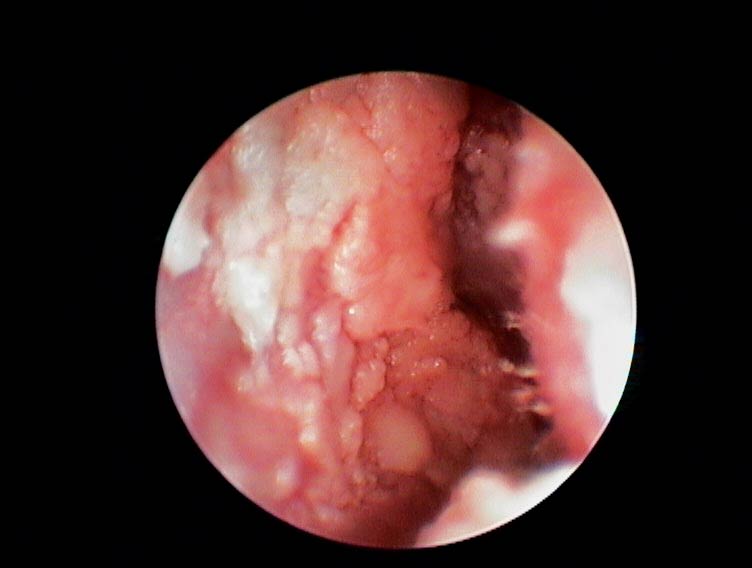
Figure 11. An endoscope can be used to confirm all the infection and lining has been removed.
In part one of this article (VT43.13), the author looked at approaches to the clinical history and diagnosis of otitis in rabbits. Part two looks at treatment options.
Otitis externa is often treated medically in rabbits. In contrast to dogs, many cases can respond to treatment, because ceruminous gland hyperplasia does not occur in response to otitis externa.
However, lop breeds are predisposed to otitis due to their anatomy and the canal is often stenotic. Proliferation of tissue may be present (Figure 1) and a biopsy for histopathology and culture is advised. Treatment includes aggressive systemic antibiotic therapy for a protracted period (typically six weeks), ear wicks soaked in antibiotics (Figure 2) or ear drops combined with topical cleaning and flushing of the ear (Figure 3; Mayer, 2011).


Ear wicks and flushing the canal can lead to inflammation and inadvertent rupture of the tympanic membrane, spreading infection into the middle ear. However, if topical therapy or ear wicks are to be used then flushing is important to increase the effectiveness of treatment. Ear wicks are placed in the ear canal after it has been cleaned and dried and should be replaced every five to seven days. These need to be cut to 75 per cent of their original length to get them seated well down the vertical canal. Once placed, topical therapy is applied daily to keep them moist. Systemic analgesics should be administered as this condition is painful. Repeat otoscopic or endoscopic examination is essential to evaluate the success of treatment.
Presumptive antibiotic therapy can be administered and bactericidal agents likely to be effective against Pasteurella multocida should be chosen, but it is wise to ensure anaerobic cover as well. Common agents used include narrow-spectrum penicillins (parenterally) or enrofloxacin (parenterally or orally). Cultures can be taken from material in the external ear canal or at the time of surgery if needed. Aerobic, anaerobic and fungal cultures should be requested. If medical treatment fails, then surgical intervention is required.
Otitis media can be treated medically, following a similar regime to that used for otitis externa. Cultures can be taken endoscopically via a needle passed through the tympanic membrane or taken from material in the vertical canal. Myringotomy has been suggested as a method treatment, allowing drainage of the purulent material from the otitis media (Mayer, 2011). Medical treatment is unlikely to be successful due to the large amount of solid purulent material within the bulla itself, and surgical intervention is recommended.If vestibular signs are present (due to otitis interna), prochlorperazine can be used. This is a phenothiazine derivative that acts on the vestibular nervous pathways. Benzodiazepines, such as diazepam, can be used to suppress acute neurological signs. Despite confinement being necessary for rabbits at risk of traumatising themselves, rabbits respond to treatment more quickly and better if they are attempting normal activity and feeding.
Metoclopramide has also been used due to its central actions. If medical treatment has been attempted then repeat evaluation is required and CT would be the best option to consider. If solid soft tissue density material is still identified in the bulla, surgery is indicated. The infection may simply persist in the bulla but not in the bone (there may not be an osteomyelitis present), but in either case the solid material will require surgical removal.

If a practitioner is planning surgery, careful meticulous technique is required to minimise the risk of complications and recurrence.
Reviewing the anatomy on a prepared rabbit skull is useful prior to surgery.
Magnifying surgical loupes are incredibly helpful for these procedures (Figure 4). There are a number of surgical treatment options generally comparable with those used for canine and feline species, but the key anatomic and physiologic differences must be taken into account.
If otitis externa is present, without otitis media, then a lateral wall resection (LWR) can be performed.
In dogs and cats the lateral wall of the vertical canal is removed and an opening created at the end of the horizontal canal. This procedure increases ventilation and drainage of the ear canal and allows medication to be topically applied. This is less invasive than a total ear canal ablation/lateral bulla osteotomy. In dogs the outcome can be poor and in one study 55 per cent had an unacceptable outcome (Sylvestre, 1998).
In rabbits, the procedure is different because rabbits lack a horizontal canal and have a solid long external acoustic meatus. The whole of the ear is shaved and prepared surgically. Two incisions are made from the base of the ear (over the bulla) following the line of the pinna approximately 10mm apart. The subcutaneous tissue is dissected free from the cartilage of the ear canal. Incisions are made in the cartilage following these lines to the top of the vertical canal and the tissue is then reflected ventrally. The cartilage flap is then incised and removed. The skin is sutured directly on to the ear canal mucosal lining along the incisions up to the pinna.
An alternative is to create a downward flap of cartilage and suture this ventrally to ensure the section of vertical canal left is as open as possible (Figure 5). The wounds require gentle cleaning only.
This technique may not resolve the otitis externa, primarily due to the anatomy as the remaining bony acoustic meatus is still vertical, and ventilation and drainage are not achieved. Cases should be selected very carefully and ongoing treatment is likely. A total ear canal ablation is usually preferable and the LWR procedure is not recommended in rabbits (Chow, 2011; Mayer, 2011).
A total ear canal ablation and lateral bulla osteotomy (TECA/ LBO) is the recommended procedure for otitis media and otitis externa. If there is no evidence of middle ear involvement, it is still recommended the lateral bulla osteotomy is performed in refractory cases of otitis externa.
Performing the TECA can be deleterious, with the risk of infection being left behind in the external acoustic duct. If this infection progresses then there is no external canal to act as a drainage point and so the infection is likely to progress to an otitis media via the tympanic membrane. As the eustachian tube is likely to be blocked by discharge (preventing drainage) a facial swelling will develop. It is therefore safer to assume there is likely to be pathology and perform the LBO as well.
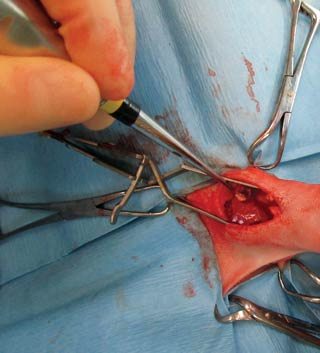
The whole of the ear is shaved and surgically prepared. A single incision is made from the ear pinna down to the base of the ear over the bulla (Figure 6). The subcutaneous tissue is separated and the vertical canal is then dissected free from this tissue and this is extended behind the vertical canal. This dissection must be as close to the canal as possible to avoid haemorrhage from the auricular artery and facial nerve damage.
A cotton bud passed into the canal will help identify the canal and enable close dissection. The top of the vertical canal is cut, which allows for the complete dissection of the canal from the ear pinna. Allis tissue forceps are applied and used to apply traction and allow fine dissection (Figure 7).



Once the vertical canal is free, the external acoustic duct can be palpated. Sharp dissection is used to free all of the cartilage from the duct, otherwise abscesses may form, creating fistulas. This reveals the external acoustic opening. If otitis externa is present this will reveal purulent material in the duct. The lateral wall of the external acoustic duct is removed using rongeurs. This opens up the entrance to the bulla and if the eardrum was intact at this point it will probably be opened by this action.
This is a hard section to remove because the entrance is only just big enough to use a fine pair of rongeurs (Figure 8). However, the bone thickness at this point and requires a much stronger instrument. Larger rongeurs work fine when held at an angle to break down the thick lateral wall. The ventral aspect of the bulla is thin and may shatter and the pieces need to be retrieved, or removed using fine rongeurs. It is important to remove as much of the lateral and ventral walls as possible, then the soft tissues can be visualised. Volkmann spoon currettes are ideal for removal of the mucosal lining and pus. At this point a culture can be taken for bacterial culture and sensitivity.





Gentle flushing should be performed at the time of surgery. This has been shown to reduce the numbers of bacteria present. In one canine study, flushing reduced positive cultures by 33 per cent (Hettlich et al, 2005). However, cultures preflushing and postflushing showed a different sensitivity pattern in 84 per cent of cases, which also were different from cultures taken from para-aural abscessation. Bacterial culture and sensitivity therefore may prove to be unreliable.Bulla endoscopy is possible to confirm all infection has been removed. It is important to avoid the facial nerve as it exits the skull from the stylomastoid foramen. It then runs along the ventrolateral aspect of the bulla.

Marsupialisation can be performed by suturing the tissues of the bulla to the skin and suturing the skin to the mucosa along the entire length of the ear canal. This does allow for postoperative flushing, but also allows for the ingress of infection and complications. Leaving the bulla open in canine patients leads to a delay in healing and increases postoperative complications (Devitt et al, 1997). Therefore, it is recommended the surgical site is closed.
Antibiotic-impregnated polymethylmethacrylate beads (AIPMMB) can be placed into the bulla. These provide a high local concentration of antibiotic with minimal systemic absorption, but this procedure is not commonly performed in other species, with meticulous surgery being the preferred option (Chow, 2011). Beads are typically made from gentamicin bone cement with the addition of other antibiotics to extend the spectrum of activity. The potential ototoxicity of the gentamicin is a concern and so this author prefers to avoid the use of beads.
Closure is performed using poliglecaprone 25. The tissues at the top of the wound are closed in a T-shape, but it is difficult to retain normal aural anatomy. There is a tendency for the ear to be tilted laterally.
A single ventral bulla osteotomy case has been described and advocated for cases with otitis media without otitis externa, as there is no access to the external ear canal with this technique. This allows removal of debris and epithelial lining within the bulla and ventral drainage, or the placement of beads is possible via this route if the surgeon wishes. Rabbits have a wide mandible, which makes lateral palpation of the bulla difficult (once you know the anatomy this is not a problem) and a thick lateral wall of the tympanic bulla (which can be circumvented), but still, this technique has been advocated as an alternative (Chow, 2011).
The ventral aspect of the mandible is surgically prepared. The entry point is parallel and medial to the mandible and mandibular salivary gland and lateral to the digastricus muscle. This is separated from the hyoglossal and styloglossal muscles, while avoiding the hyoglossal nerve. The bulla can be palpated deeper in the tissues (dorsally) and dissection reveals access to the ventral aspect. The jugular process of the skull lies laterally to the point of incision. A small intramedullary pin is used to gain entry and the hole is enlarged with rongeurs. Potential complications are identical to those for the TECA/LBO.
A newer technique has been developed at the University of Edinburgh Royal (Dick) School of Veterinary Studies, which simplifies these procedures and reduces patient morbidity associated with ear surgery and retains the cosmetic appearance of the rabbit. In cases with otitis media and otitis externa there is minimal pathological change in the dorsal vertical canal and removal of this tissue is excessive and closure time is extended as a result.
The new technique requires a shorter incision at the ear base (Figure 9). The subcutaneous tissue is dissected down to the vertical canal and this is carefully dissected free of surrounding tissue (keeping close to the cartilage). The vertical canal is then bisected and the lower portion is grasped with Allis tissue forceps at the top, holding the canal closed. This is then dissected free down to the external acoustic duct. Sharp dissection is used to free all the cartilage from this.
From this point on the surgery of the bulla proceeds as described above and purulent material is removed (Figure 10). Endoscopic examination of the bulla can be used to confirm all the infection and lining has been removed (Figure 11). All tissues are closed with poligecaprone 25. The mucosa of the vertical canal is accurately opposed and the cartilage closed with a horizontal mattress suture, essentially creating another blind-ending pouch. The remaining soft tissues are closed and the skin closed using a subcuticular pattern (Figure 12). Cosmetically, these rabbits appear perfectly normal after the procedure.

Pre-emptive analgesia is important and a pure mu opioid is required, such as fentanyl or morphine, with additional analgesia provided by meloxicam and a local block in the incision with lidocaine and bupivacaine. During surgery, a continuous rate infusion (CRI) of ketamine and dexmedetomidine can be given. Postoperatively, morphine is used alongside the CRI. This is followed by buprenorphine and further meloxicam. Antibiotic therapy should ideally be based on culture and sensitivity taken from the bulla at the time of surgery, despite the limitations outlined above. As a result, antibiotic therapy postoperatively can be empirically chosen. Antibiotics such as enrofloxacin, penicillin or sulphonamides may be chosen. Six weeks of therapy is recommended.
Complications include facial nerve paresis or paralysis, resulting in loss of palpebral reflex, exposure keratitis and an inability to move the muscles of the face or facial nerve spasticity, due to inflammation around the nerve after surgery (Figure 13).
Vestibular dysfunction (head tilt, nystagmus and torticollis) can present if otitis interna has occurred. This may be due to excessive curettage in the dorsomedial aspect of the bulla damaging the promontory, vestibular and cochlear window or due to pressure from postoperative flushing. Tongue paralysis is also possible due to hypoglossal nerve damage. Horner’s syndrome is also possible and presents as miosis, ptosis and enopthalmos. Haemorrhage is possible due to damage to the rostral auricular artery. Oedema of local tissues is possible due to disrupted lymph flow (Figure 14).
One of the main concerns is recurrence of the infection, leading to abscessation or fistulous tract formation (due to failure to remove all of the epithelial lining or a bone fragment). This generally becomes apparent within six to nine months postoperatively. Repeat surgery is indicated if infection becomes evident.
Evaluating the middle ear for recurrence of infection is difficult as the surgical site should fill with granulation tissue postoperatively. CT examination will demonstrate a soft tissue density within the surgical site. If there are bone changes, or a soft tissue swelling is noticed laterally under the ear base, then recurrent infection is likely (Figure 15).
Careful meticulous tech nique, with magnification, will help minimise the rate of complications and referral for the diagnosis and surgery may well be the best approach. Facial nerve spasticity is the most frequent postoperative complication, but is usually transient.
Rabbits with head tilts and nystagmus should undergo CT examination as soon as possible to enable appropriate therapy to be undertaken. In the case of otitis media, surgical intervention is indicated to maximise the chances of success.