17 Mar 2026
Glen Cousquer BSc(Hons), BVM&S, CertZooMed, PGDOE, MSc(Outdoor Education), MSc(Education Research, PhD IML, PFHEA, MRCVS talks about this important issue from a health and safety perspective.
Glen Cousquer
Job Title
Image: Pixel-Shot / Adobe Stock
As the RCVS brings in new rules requiring practices to have their own specific suicide prevention plans (Loeb, 2026), this feature applies an occupational health and safety lens to consider the challenge of providing a safe working environment for health care professionals.
It starts with an overview of the field of occupational health and safety, and explores two relevant international and national standards that have been developed in recent years on psychosocial safety, stress risk management and suicide prevention in the workplace.
This feature applauds the initiative taken by the RCVS, for it represents a clear recognition that suicide prevention plans should be integrated into practice standards. At the same time, the author takes issue with the failure of the profession to engage with broader occupational health and safety principles, and to learn from the decades of work in other sectors that have led to the development of a wide range of standards for integrating risk management for mental health, alongside those developed for the management of physical health risks.
This work has been both driven and supported by the trade union movement, and health and safety bodies (Johansen and Partanen, 2002; Lucio, 2020; Vesper et al, 2025), who recognise that work-related stress has become the most significant workplace health priority, as reflected in the UK Health and Safety Executive’s current 10-year strategy (HSE, 2022). An occupational health and safety approach recognises the need to organise all mental health interventions based on the prevention level they are designed to address (Calvet et al, 2021; Davis and Morganson, 2019a; 2019b; Obas et al, 2022).
Any discussion of suicide needs to recognise this bigger contextual picture and the possibility of intervening more strategically and comprehensively. As part of this, we need to recognise that a societal paradigm shift is needed to allow a systems approach to addressing mental health and suicide to be developed. The UK, for example, is one of only 38 countries to have a suicide prevention plan and yet, as Waters and Palmer (2022) point out, the country’s health and safety legislation and general approach are woefully out of date, as outlined by the following:
Across the globe, in France, Japan and the US, clear recognition exists of the need to recognise, record and investigate work-related suicides. Both Australia and New Zealand have recently amended their reportable incident regulations to include suicide. This reflects current understanding of how to define work-related suicides, with LaMontagne et al (2024) identifying “the threshold for determining work-relatedness as adequate evidence to justify policy or practice action, an approach informed by the precautionary principle”.
The veterinary profession in these countries will be evolving their approach to suicide within these legal frameworks. In France1, for example, the tragic suicide of a number of staff and students at the national veterinary school of Alfort will not have been treated as a private matter, but reported to the relevant authorities. The UK is not so fortunate (Waters and Palmer, 2022).
Arguably, the veterinary profession in the UK needs a more holistic strategic approach and better data in this area (Cousquer, 2023; Cousquer et al, 2025). This is, in part, because the sector has had limited input from occupational health and safety professionals. In what follows, we consider the current legal background of mental health in the workplace and the recent publication of BSI 30480 and ISO 45003. This allows us to consider how relevant legislation, codes of practice and guidance can inform the development of approaches in this area. A key lesson emerging from this overview is the need for an occupational health and safety approach that recognises the need for primary, secondary and tertiary measures to be part of any strategy going forwards. The article concludes with some simple suggestions that can be explored as we continue to evolve our approach in this area.
A health and safety approach to tackling workplace mental health (and especially workload and work-related stressors) should focus on developing collective solutions through an organisation-level stress risk assessment, which an employer must develop as part of its responsibilities under Regulation 3 of the Management of Health and Safety at Work Regulations 1999.
The Trades Union Congress (TUC)2 and Hazards3 argue that employers must address the root cause of all work-related stressors such as excessive workloads, high pace and intensity of work, long working hours and lack of work-life balance. Alongside therapeutic measures designed to target individual workers, they should address the structural and organisational conditions of work. Many employers, however, fail to focus on the root cause of workload stressors in their workplaces and do not develop the corresponding primary interventions that will manage these stressors.
Instead, they focus on the worker, prioritising secondary and tertiary interventions4. As such, it is probably fair to say that most employers will not be meeting the legal minimums to ensure compliance under health and safety legislation. Prioritising work centred around changing the individual workers and making them more resilient to stress without first looking at changing the work itself needs to be called out as a failure in responsibility.
These legal minimums are outlined through the Health and Safety at Work etc. Act 1974, which is the primary piece of legislation covering occupational health and safety in Great Britain. Employers must operate within the legal framework in the UK to ensure employees are safe and protected from harm while at work. Employers also have a legal duty to consult with trade union health and safety representatives in recognised workplaces on all significant safety matters under the Safety Representatives and Safety Committees Regulations 1977. This is an area that the veterinary profession arguably needs to consider more closely, recognising that unionised workplaces in which trained safety representatives receive the facility time they are legally entitled to, to fulfil their duties, are safer workplaces.
The Management of Health and Safety at Work Regulations 1999 (Great Britain), and the Management of Health and Safety at Work Regulations 2000 (Northern Ireland), detail how employers must conduct suitable and sufficient risk assessments (Regulation 3), following “principles of prevention” (Regulation 4) to avoid or mitigate against any potential risks to workers’ health, safety and welfare. A systematic, robust approach to preventing workplace stress, following a systematic approach to risk assessment, will allow employers to:
The process of assessing the risks associated with work-related stress should follow the five-step approach to risk assessment5, starting with the identification of hazards. For this, they can use the six key areas of work design identified in the HSE management standards6: demands, control, support, relationship, role and change. By focusing on these, the main stress risk factors specific to the workplace can be identified, while remaining mindful that these categories of risk often overlap, combine or interact.
It is important that employers focus on the prevention of workplace stress by tackling the root causes. This necessitates an organisation-level approach to the risk assessment process. Specific workplace stress risk factors can be identified via a number of different mechanisms:
ISO 45003 provides guidance for managing psychosocial risk within an occupational health and safety management system, based on ISO 45001.
Launched in 2021, this is the first international standard dedicated to psychological health and safety at work. It provides practical guidance on identifying and managing excessive workloads, poor communication, job insecurity, workplace bullying and other psychosocial risks.
The core concepts recognise that:
It is likely that engaging with this standard will support organisations in managing mental health risks in the workplace, including the risk of suicide. This, however, represents a very specific risk and it is, therefore, reassuring to know that the British Standards Institute has just published BS 30480, which specifically seeks to summarise the measures organisations can take for suicide prevention, intervention, and support for those affected by suicide, providing “guidance on creating and sustaining safe, supportive work environments where people can thrive and survive in life and through crises” (BSI, 2025).
It is particularly reassuring that this standard is freely available and up to date, and that it has been written for all workers, including managers, human resources teams, health and safety teams and occupational health teams, as well as those in organisational health and well-being, diversity and inclusion, and learning and development.
It will be particularly valuable to those who are responsible for managing performance, workload, mental health and well-being and work environments.
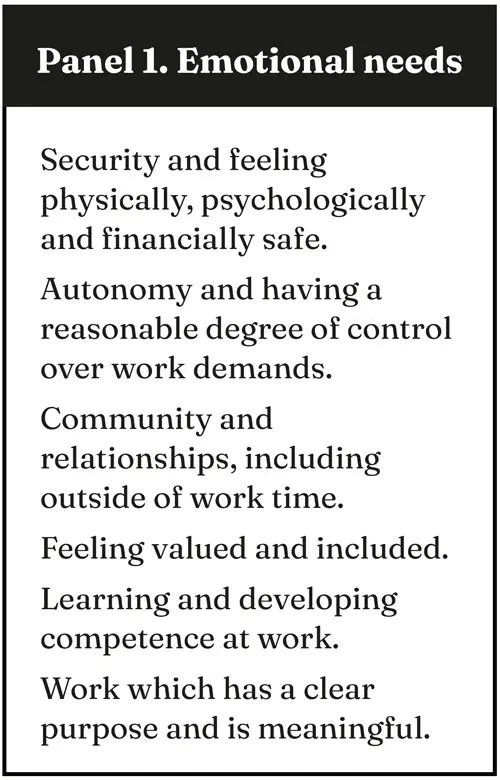
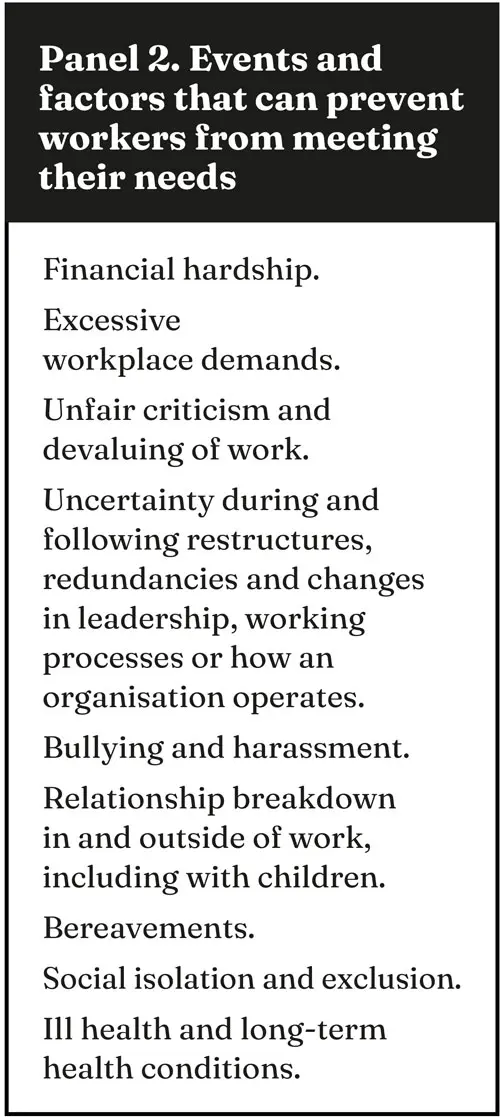
The reader will not be surprised to learn that BS30480 places a strong emphasis on organisational culture. Such cultures allow workers to meet psychological needs (Panel 1) in healthy ways, recognising the extent to which these make a significant contribution to preventing suicide and enabling workers to ask for support if they are experiencing thoughts of suicide. Organisations should, furthermore, be aware of when events and factors in the workplace prevent workers from meeting their needs (Panel 2).
It is only later in the standard, under section 6.6, that reducing access to means of suicide is addressed. This reflects the order of priorities an occupational health and safety approach emphasises and should take.
According to Loeb (2026), the RCVS “defines a suicide prevention plan as ‘a collection of measures which aim to protect staff and the wider public by reducing incidences [sic] of suicide’.” It says each plan should be bespoke and tailored to the specific practice, while also acknowledging that risk mitigation measures must be balanced against “allowing the practice to deliver care appropriately”.
It says areas covered by the risk assessment should include storage of certain veterinary medicines, access to firearms and lone or late-night working.
Mitigation measures may include protocols for access to and handling of some items, having mental health first aiders on site and the use of some Vetlife resources, including a poster signposting anyone needing to talk in confidence to the Vetlife Helpline.
This account would appear to suggest that a risk assessment or prevention plan focuses on tertiary measures, including managing access to a means of suicide and promoting access to helplines and mental health first aiders. This would suggest that a lot of work remains to do to understand both suicide prevention and the prevention of poor mental health in the workplace.
The good news is that section 5.0 of the standard provides clear guidance on the development of a comprehensive strategy and policy for preventing suicide.
A coordinated framework of strategy, policies, implementation plans and monitoring is strongly recommended. The strategy describes the organisation’s vision and demonstrates its commitment to delivery. As part of this, buy in from senior management, established accountability and clear resource allocation must all also be present.
Policies translate the strategy into specific principles, procedures and responsibilities, detailing how the strategy will be delivered. Implementation plans set timelines and structures for delivering the overall strategy and associated policies.
Lastly, monitoring supports organisations in regularly reviewing and evaluating the effectiveness of their strategy, policies and plans, enabling actions to be taken to ensure allocated resources are sufficient, progress is made and that the strategy, policies and plans remain effective.
This feature has highlighted developments in the field of occupational health and safety that are highly relevant to the progress the veterinary profession needs to make in delivering psychosocial safety in the workplace and effective stress-risk management.
As part of this work, suicide prevention strategies and plans can be developed that will integrate the right balance of primary, secondary and tertiary interventions. This feature has highlighted the value of engaging with the ISO 45003 and BSI 30480 standards, and the need to invest in capacity building. Such investments arguably need to be collaborative, involving both staff representatives and management.
Readers interested in exploring these possibilities can download BSI 30480 from the link in the references section. The document is free to download and offers clear guidance for organisations of all sizes and sectors, from public bodies, charities and social enterprises to businesses and commercial enterprises.
This feature has also emphasised the crucial role that union safety representatives can play in advocating for change. Employees can ask their union to appoint them as a safety representative; they then are legally entitled to time as necessary for training and to perform their duties. This can be a game changer, empowering employees to assert their legal right to safe working practices, environments and cultures, and hold management to account.
A collaborative approach is best achieved through the creation of a health and safety committee within the workplace, something that should be achievable within all corporate practices and even in smaller practices.
Looking to the future, this is one area that could be integrated into future revisions of the Practice Standards Scheme to ensure that oversight of suicide prevention plans and other approaches to staff mental health and well-being are undertaken collaboratively, and recognise the need for a tiered approach.
Glen Cousquer is an interdisciplinary scholar who works across a wide range of disciplines, lecturing in one health and conservation medicine at The University of Edinburgh’s veterinary school, where he is also chairperson of the mental health and well-being committee. He was awarded principal fellowship of the Higher Education Academy in 2025 for his strategic leadership in biodiversity and mental health literacy across the higher education sector. Glen is also a writer, photographer, international mountain leader, mindfulness teacher and veterinary surgeon. His interests include deep ecology, environmental education, ecological approaches to veterinary medicine, one health approaches to animal welfare and wild animal medicine.
1. For more on the approach taken in France, visit tinyurl.com/3jm8556f
2. The TUC website provides access to a wealth of reports on health and safety in the workplace, including an annual safety representatives survey. Available at tinyurl.com/3jr88f9p
<em>3. Hazards</em> is an independent, union-friendly magazine providing the information and resources to support union safety representatives. It looks behind the company safety hype and gives union answers to workplace problems. Available at tinyurl.com/3xsv7nvs
4. Primary measures focus on preventing mental health conditions before they develop by addressing risk factors; as such, the focus is on the work undertaken. Secondary measures encompass approaches that involve early detection and identification of emerging mental health conditions; as such, the level of harm is minimised. Tertiary level encompasses approaches that focus on reducing the impact of mental health conditions through careful management.
5. For more on managing risks and risk assessment at work, visit tinyurl.com/bdftr5me
6. For more on management standards, visit tinyurl.com/yz9pbsvu