19 Nov 2018
Jane Davidson kicks off #PlanVetRVN and encourages vets and VNs to delegate work better within the team to provide less stress for vets, better job satisfaction for nurses and better results for patients.
Jane Davidson
Job Title
I’m sorry if it looks like November is Schedule 3 (SIII) month for my blog, but I’ve had both posts brewing for some time and other more timely blogs have always taken precedence… but here they are.
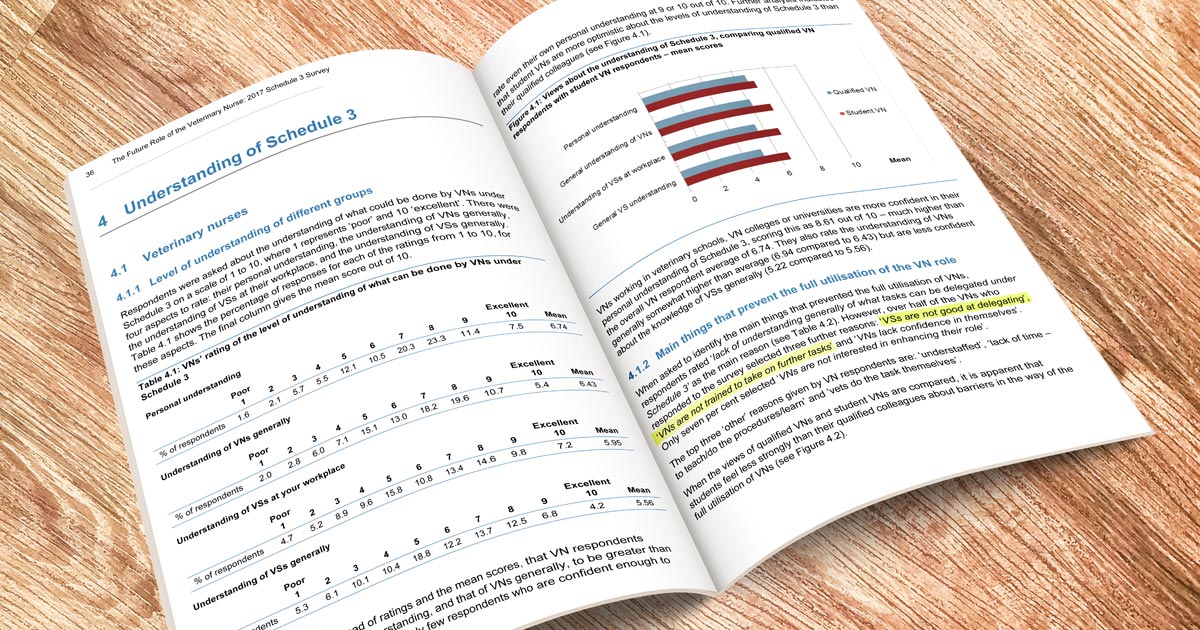
The results of the RCVS survey on SIII showed many vets aren’t sure what SIII means, which makes it difficult to delegate tasks a vet nurse can legally do.
That’s understandable as you need to have a full understanding of another professionals’ role, and while there are discussions at practice level, and regulatory and representative level, some confusion exists – so let’s take a look at current regulation for RVNs.
SIII is an amendment to the Veterinary Surgeons Act and occurred in 2002 – check the details here or use my handy summary.
18.4
Under this Schedule 3 exemption, the privilege of giving any medical treatment or carrying out minor surgery, not involving entry into a body cavity, is given to:
RVNs
Wow… so that’s a lot more things to define? That is sometimes the problem – what is minor surgery or direct supervision?
Treatment required by a patient. For example:
Surgery that does not involve the major structures of the body (for example, where only skin or mucus membranes or minor connective tissue is in the operating field) – while this guide suggests minor surgery is the correct term for surgery carried out in a body cavity that has “immediate access with the outside world”, perhaps this definition could be used in the future?
There is no surgical procedure in a body cavity:
Common examples of legal vet nurse minor surgery include:
As it seems to be the minor surgery part of SIII for RVNs that leads to the most confusion, I’ll focus on that.
I’m going to add a note of caution here – there is no exhaustive list of all the duties an RVN can do under SIII, but these can be taken rather as a starting point for discussions between the team, or check the EMS guide in my last blog.
Firstly, let’s understand some more terminology.
Don’t worry if you’re not sure what direction or supervision mean:
For vets to delegate tasks properly they need to be considering their own needs, the vet nurses skills, the patient and client needs, and current legislation.
The vet nurse needs to:
The patient must:
The client must:
Current legislation
You might find published case studies from the RCVS helpful. It is our joint responsibility to understand each others’ role and skills and delegate where appropriate to help the team and the patient to the best of our abilities.

The ability to carry out any of these skills and others that may fall under the remit of SIII are privileges – the RCVS states this, and I believe it is the best attitude to take when approaching this area.
Further training and support is required for everyone involved to ensure using SIII skills is the best thing for the team and the patient.
For many VNs, an employer that allows a range of SIII procedures and knows they are very appealing. If you use even just some of the skills possible in SIII, this can create better job satisfaction for the nurses, it can reduce the stress on the vets and it promotes a great team atmosphere.
As a vet and vet nurse you can ask yourself some questions before delegating or accepting delegation:
We need to work together to improve the working lives for the whole team. Less stress for vets, better job satisfaction for nurses, better results for patients – these aren’t mutually exclusive.
It may help to start discussing delegation during team meetings or when reviewing standard operating procedures, so, as a team, you all understand what skills are suitable for delegation in your team.
Let’s work together and start #PlanVetRVN.