13 Nov 2017
Belinda Rose discusses the use of ovulatory induction agents and post-covering treatments in reducing early pregnancy loss in horses.
Belinda Rose
Job Title
Image: Fotolia/kwadrat70.
Ovulatory induction agents are used in more than 90% of Thoroughbred broodmares, and post-covering treatments in more than 60% of mares. Despite this, corresponding improvements in pregnancy rates and live foal rates have not been recognised. Evidence does, however, suggest physiological benefits may exist relating to the use of ovulatory induction agents conferring protection to the early conceptus, with a reduced incidence of early pregnancy loss associated with their use.
The use of flunixin meglumine at the time of manual reduction of twin pregnancies has also been shown to reduce the incidence of early pregnancy loss. Conversely, little evidence exists to justify the widespread treatment of broodmares post-cover, although intrauterine lavage post-cover has been associated with a significantly enlarged conceptus between gestation days 11 to 34. Also, little evidence exists in support of altrenogest post-cover, other than in the face of a known luteal insufficiency; however, the use of a single dose of buserelin at around gestation day 10 is associated with improved early pregnancy rates.
Multivariable analysis, taking into account mare age, has found the presence of uterine cysts to be associated with an increased incidence of early pregnancy loss. Treatment of these structures appears to be warranted.
The use of pharmacological agents in broodmare management in the UK and Ireland has risen substantially in the past 20 years.

In the Thoroughbred industry, at least, factors propelling this change include the growing book sizes of popular sires, use of dual hemisphere stallions and desires for early-season foals. These pressures have led to the increasing use of therapeutic interventions to help minimise the number of covers per mare and maximise the success of early season matings.
While improvements relating to early season matings and a lower number of covers per oestrus may result from these increases, improvements in pregnancy and live foal rates remain broadly unaltered. The first cycle pregnancy rate detected over the 2008-9 breeding seasons was 68%1, which compares closely to the 65% first cycle pregnancy rate over the 2002 season2. Likewise, the incidence of loss between days 15 to term was 13.5% during the 2002 season and 13.9% in the 2013-14 seasons.
Two large-scale epidemiological investigations in the UK documented the use of therapeutic agents and reproductive efficiency in Thoroughbred broodmares in the 1998 and 2002 breeding seasons2,3. A further epidemiological study by the author (awaiting publication) of more than 2,000 pregnancies in Thoroughbreds in the Newmarket area, over the 2013 and 2014 breeding seasons, has enabled a comprehensive evaluation of changes in the veterinary management of broodmares, together with an assessment of the benefits these changes have conferred.
One of the most dramatic changes seen relates to the use of human chorionic gonadotropin and deslorelin to induce ovulation.
In 1998, 49% of ovulations were allowed to occur spontaneously. By 2002, this had reduced to 41% and by 2013-14, just 8% of pregnancies resulted from natural ovulation. While the major driving force behind this relates to the ability of agents to minimise the need for repeated covers – by ensuring ovulation occurs at the time of cover – evidence suggests additional benefits may be conferred to the early conceptus, perhaps providing further justification for their use.
Enhanced serum progesterone levels to day 15 of pregnancy have been shown with the use of these agents for ovulation induction, with increased ovarian vascular perfusion and luteal blood flow also documented. Multivariable analysis, taking into consideration a range of factors, found the use of these agents to be associated with a reduced incidence of early pregnancy loss between days 15 to 65 of pregnancy, possibly as a consequence of the aforementioned findings (Figure 1).

Additional work has suggested they are capable of enhancing early conceptus growth, with vesicles in which ovulation was induced found to be significantly larger on routine ultrasound examination between gestation days 11 to 34 than those from a spontaneous ovulation.
While further work will allow a more comprehensive understanding of the mechanisms underlying these findings, it appears genuine physiological benefits are derived from their use.
Persistence of post-mating endometritis five days after ovulation results in exposure of the early embryo to a hostile intrauterine environment detrimental to fertility and, while low volumes of intrauterine fluid have not been found to adversely affect pregnancy, volumes of 2cm or greater have been associated with reduced pregnancy rates. The use of ecbolic agents, such as oxytocin and carbetocin, and intrauterine antibiotics in these cases is, therefore, certainly warranted.
Controlled studies have reported additional benefits in relation to pregnancy rates secondary to the use of antibiotics and oxytocin at cover4; however, these findings have not been replicated in clinical studies.
More than 60% of mares receive at least one treatment at the time of cover – an increase from 36% in 2002. Intrauterine antibiotics were found to be used in 50% of mares, ecbolic agents in 50% and intrauterine lavage in 24%.
Dexamethasone is also occasionally used as a post-covering therapy. The use of 50mg of dexamethasone IV at the time of breeding, in addition to other post-breeding therapies, has been shown to lead to improved pregnancy rates in problematic mares, with three or more risk factors for pregnancy failure5.
Persistent post-mating endometritis is recognised to occur in 10% to 15% of mares, and 10% of mares investigated in 2013-14 were found to have intrauterine fluid volumes greater than 2cm post-cover.
The high proportion of mares receiving post-covering therapies has suggested a conflict between the increasing recognition for a need for prudent antibiotic usage and evidence-based medicine, and needs to use all available avenues in attempts to maximise reproductive success.
Little clinical data exists to support the use of aggressive management in this wider population of broodmares. However, findings show the use of intrauterine lavage from four hours post-cover – leading to improved early embryonic growth up to gestation day 34 – are worthy of discussion.
The mechanisms behind these increases in vesicle size can only be speculated. It is possible a dilution of inflammatory debris allows for improved uptake of histotrophic nutrition. In mares with an absence of a clear need for aggressive post-covering therapy, innocuous intrauterine lavage treatment may offer a reasoned compromise for clinicians wishing to offer a post-covering treatment or facing pressures from stud staff to treat.
A meta-analysis of six equine studies found a single dose of 20µg to 40µg of buserelin, on day 8 to 12 of gestation, is capable of improving pregnancy rates by approximately 10% from days 13 to 42 of pregnancy6.
A similar improvement is seen in relation to its use in cattle. The physiological processes behind this are unclear and, while the use of gonadotropin agents in early pregnancy has been shown to enhance serum progesterone levels until day 30 of pregnancy, the benefits of enhancing early progesterone levels are controversial. Nevertheless, regardless of the causal physiology, clear evidence supports the use of a single dose of buserelin for problematic mares in this time frame.
The use of altrenogest to support pregnancies is still contentious, although often resorted to in mares with a known history of pregnancy loss or in light of a finding of a small-for-age vesicle. While its use is justified in light of a known luteal insufficiency, cases such as this are rare. The release of prostaglandin F2α – secondary to endotoxin release – is well documented, and progesterone supplementation and luteal support in cases of a known insult may certainly help. However, no clear evidence exists otherwise to support its use in rescuing failing pregnancies or enhancing conceptus growth.
The modest increase in the occurrence of multiple pregnancies – from 10.5% in 2002 to 16.1% – has raised concerns with regards to the success of the ongoing pregnancy.
This increase is likely a result of the increased usage of ovulatory induction agents. Findings have showed no associations linking the manual reduction of twin pregnancies to increasing incidences of pregnancy loss. Hence, as long as precautions are taken to ensure twin pregnancies are detected and managed accordingly, this should not be a cause for concern with regards to the subsequent pregnancy outcome.
Close attention should be paid to ensure second ovulations do not go undetected. If it is felt a second ovulation may have occurred, a day-18 scan to rule out the presence of a second pregnancy is essential.
The release of prostaglandin F2α from the endometrium – secondary to manual reduction of an embryonic vesicle – is well documented, with the volume released directly relating to the pressure required to cause embryonic rupture7.
Flunixin meglumine is often used at the time of manual reduction to inhibit this endogenous prostaglandin release; however, studies investigating the success of this treatment have yielded conflicting results. Multivariable analysis of the data collected as part of the author’s 2013-14 study found its use to significantly reduce the incidence of early pregnancy loss by nearly two-thirds, so its use in nearly 60% of mares undergoing manual reduction of a twin pregnancy appears justified.

With the prevalence of uterine cysts increasing significantly in respect to mare age, early reports have concluded the presence of cysts had no effects on fertility once mare age had been accounted for.
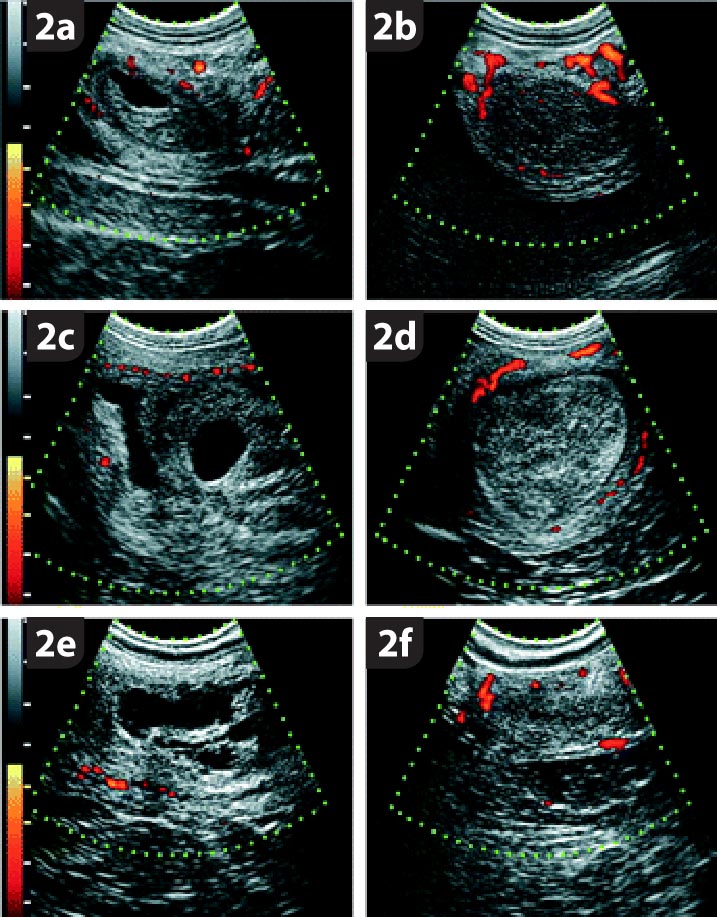
However, mares with uterine cysts have been demonstrated to have reduced uterine vascular perfusion, and a positive association has been shown between the size of the cystic area and disturbed uterine haemodynamics (Figure 2).
Two investigations, using multivariable analyses, found a positive association between the prevalence of cysts and the incidence of early pregnancy loss9, and they have been implicated in impeding vesicle migration, fixation and placentation.
The effect of the location, size and number of the cystic structures likely also plays a role in their significance, so future studies are required to better assess these variables to allow clinicians to make more accurate prognostic evaluations. In the meantime, treatment is warranted for mares with large or numerous cysts, or a poor reproductive history (Figure 3)10.
The increasing usage of therapeutic interventions in broodmares has not only economic repercussions, but also ethical, welfare and safety implications11.
Consideration of recent investigations relating to the use of reproductive therapies are, therefore, essential to ensure an evidence-based approach, to maximise reproductive success while minimising unnecessary interventions.