24 Jul 2017
This article provides a summary of selected clinically relevant publications on diagnostic methods, imaging and rehabilitation of equine lameness published in the past 12 months, as well as new information related to diagnostic imaging of the suspensory ligament.
Annamaria Nagy
Job Title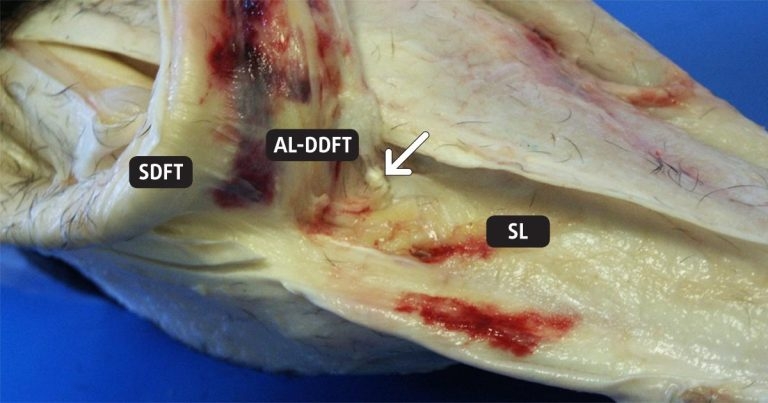
Figure 1. Gross postmortem specimen of a hindlimb of a horse with proximal suspensory desmopathy. Proximal is to the left. The flexor tendons and the accessory ligament of the deep digital flexor tendon (AL-DDFT) are reflected proximally; the suspensory ligament (SL) is left in situ. Fibrous adhesions between the SL and adjacent soft tissues (arrowed). SDFT: superficial digital flexor tendon.
The specificity of diagnostic analgesic techniques has been of continued interest. Jordana et al (2016) investigated diffusion of mepivacaine to adjacent synovial structures after intrasynovial analgesia of the digital flexor tendon sheath (DFTS).
Synoviocentesis of the DFTS was performed using the palmar/plantar axial sesamoidean approach in eight horses under general anaesthesia and 1ml/50kg (9.4ml to 13ml) mepivacaine was injected.
Mepivacaine concentration was measured 15 and 60 minutes after injection in the ipsilateral metacarpo/metatarsophalangeal joint, proximal and distal interphalangeal joints, navicular bursa and contralateral metacarpo/metatarsophalangeal joint. Mepivacaine was detected in all synovial cavities, but in very low concentrations, which would not be sufficient to provide analgesia.
Mepivacaine concentration in the jugular vein was lower than in the ipsilateral synovial cavities, but higher than in the contralateral metacarpo/metatarsophalangeal joint. This indicated systemic absorption of mepivacaine from the DFTS, but the low systemic concentrations were insufficient to result in diffusion into other synovial structures.
The authors suggested presence of mepivacaine in adjacent synovial structures was probably the result of local diffusion rather than of systemic distribution. This hypothesis is, however, not supported by the fact, at 15 minutes, no significant difference is seen between mepivacaine concentration in the ipsilateral and contralateral metacarpo/metatarsophalangeal joints.
Diagnostic analgesia of the digit (including perineural analgesia of the palmar and palmar digital nerves) is much less specific than once thought.
Paz et al (2016) tested the hypothesis the dorsal laminae of the foot are innervated by the palmar digital nerves and not by the dorsal branches or the palmar nerves. They assessed mechanical nociceptive thresholds in several parts of the foot of six clinically normal horses before and after perineural analgesia of the palmar digital nerves and the dorsal branches of the palmar nerves (performed separately).
Perineural analgesia of the palmar digital nerves distal to the dorsal branch of the palmar nerve did increase the mechanical nociceptive threshold, not only in the bulbs of the heel, but also in the dorsal laminae and the sole. Perineural analgesia of the dorsal branches of the palmar nerves only increased the nociceptive threshold at the level of the coronary band.
This study highlights that if lameness improves following palmar digital nerve blocks, the dorsal, and not just the palmar aspect of the foot, including the dorsal laminae, should also be considered as potential sources of pain.
It should be borne in mind laminar damage is not only seen in association with the typical marked signs of laminitis. Laminar damage can be mild, resulting in mild lameness and/or poor performance and, in some cases, diagnosis may only be achieved by MRI.
Compensatory forelimb lameness in horses with hindlimb lameness is well recognised. A study by Maliye and Marshall (2016) established, using objective gait analysis, that hindlimb lameness can result in ipsilateral, but not contralateral, forelimb lameness. The study included 37 horses with unilateral hindlimb lameness, with or without ipsilateral or contralateral forelimb lameness.
Authors compared head and pelvic movement asymmetry before andafter diagnostic analgesia of the lame hindlimb. Head movement asymmetrywas significantly decreased after diagnostic local analgesia in horses with hindlimb and ipsilateral forelimb lameness, and for all horses combined, but not in horses with hindlimb lameness only, or those with hindlimb and contralateral forelimb lameness.
These results support that hindlimb lameness can cause compensatory load redistribution, which can manifest as apparent forelimb lameness. In this study, contralateral forelimb was not compensatory and likely reflected genuine forelimb lameness, confirming previous subjective clinical observations.
Studies comparing ultrasonographic and MRI findings in the proximal aspect of the suspensory ligament (SL) have suggested ultrasonography was unreliable in the detection of hindlimb proximal suspensory desmopathy (PSD).
Dyson et al (2017) validated ultrasonographic examination of PSD in the hindlimb against gross postmortem and histopathological results in horses with hindlimb PSD and in control horses. They also examined three horses with recurrent lameness following surgical management (plantar neurectomy and fasciotomy) of PSD.
Gross postmortem and histological examinations of control limbs revealed no abnormalities. Gross postmortem examination revealed substantial adhesions between the proximal aspect of the SL and adjacent soft tissues in 27% of lame limbs (Figure 1).
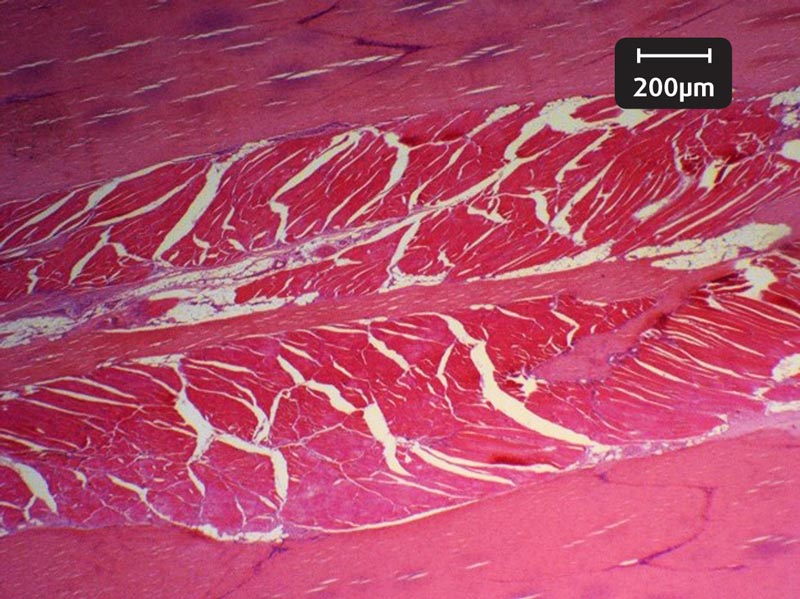
In 27% of limbs, adhesions were seen between the body of the SL and the mid plantar aspect of the third metatarsal bone, extending distally in 16.2% of limbs. Histology revealed abnormalities of the collagenous tissue in 69.4% of limbs; in the muscle in 97.2% (Figure 2) and in the adipose tissue in 44.4% of limbs.
In horses with recurrent lameness following surgery, adhesions between the SL and adjacent soft tissues were predicted ultrasonographically and confirmed postmortem. The authors concluded ultrasonography was reliable for the detection of SL pathology based on histology as the gold standard, and suggested adhesions may be a reason for recurrent lameness after surgery.
Plevin et al (2016) investigated the possible association between sesamoiditis, subclinical ultrasonographic suspensory ligament branch change and subsequent clinical injury in yearling Thoroughbreds. Fifty yearlings were evaluated at the onset of training and followed for nine months.
The forelimb suspensory ligament branches and proximal sesamoid bones were assessed radiographically and ultrasonographically. Possibly significant sesamoiditis was defined as greater than or equal to one divergent vascular channel of greater than or equal to 2mm width, with or without abaxial lucency and/or abaxial border change.
Ultrasonographic findings were classified as possibly significant SL branch change if they included extensive regions of mild hypoechogenicity and/or small focal disruptions of fibre pattern or regions of marked disruption of fibre pattern and/or large anechoic core defects.
Clinical SL branch injury was defined as the presence of pain response to palpation and/or avoidance response to direct palpation; visible swelling or palpable thickening of the branch; or focal inflammation, with or without lameness.
Eight clinical SL branch injury cases were noted; all demonstrated deterioration on ultrasound examination when compared with initial images.

The presence of possibly significant sesamoiditis alone and possibly significant SL branch changes alone were risk factors for subsequent SL branch injury. The coexistence of possibly significant sesamoiditis and possibly significant SL branch changes significantly increased the risk of subsequent development of clinical signs of SL branch injury (odds ratio 11.7).
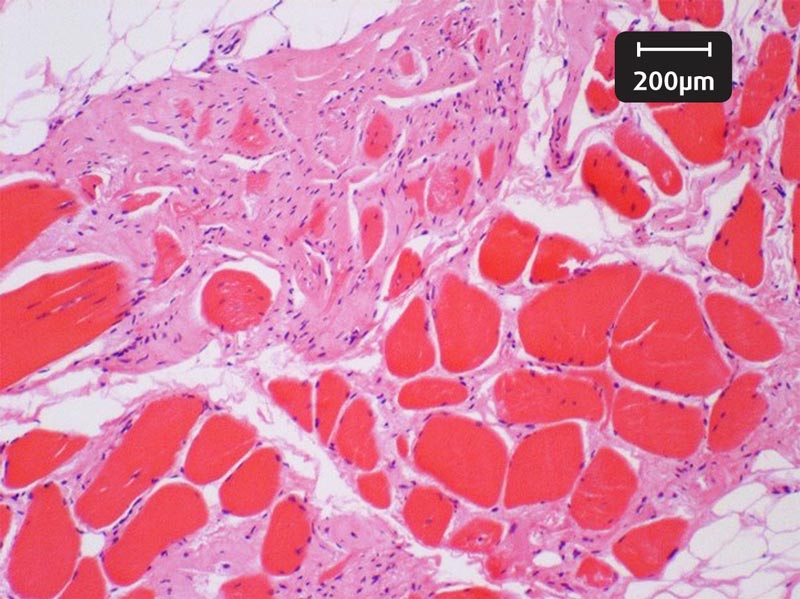
Interestingly, in National Huntracehorses, no association was seen between ultrasonographic abnormalitiesin the branches of the SL (including moderate hypoechogenicity, reduced fibre pattern and a fragment separated fromthe proximal sesamoid bone; Figure 3) and clinical injury in a study by Fairburnet al (2017).
Clinical and ultrasonographic examinations were performed, but radiographs were not obtained. In this study of 62 National Hunt racehorses, the prevalence of ultrasonographic lesions of the severity considered possibly significant in yearling flat racehorses (Plevin et al, 2016) was 30.6%. The median age of horses was five years; it is possible older horses and horses participating in National Hunt races cope better with ultrasonographic abnormalities of the SL branches than yearlings, and horses participating in flat racing only.
Radiographically identified sesamoiditis in conjunction with ultrasonographic abnormalities might have been associated with clinical injury. Fairburn et al’s study was restricted to a single examination; it is possible, with time, some of these horses might have developed clinical signs of suspensory branch injury.
While a large number of papers are being published on the diagnosis of various orthopaedic conditions, much smaller steps are being made in treating and managing injuries.
Robust, evidence-based results are still scarce – particularly on rehabilitation of specific injuries. A review on trunk and hindlimb muscle activity and exercise selection in rehabilitation highlighted the lack of, and urgent need for, research (Tabor and Williams, 2017). Any evidence for exercise selection for injury rehabilitation is anecdotal at best.
Use of a water treadmill has been gaining popularity, both as a part of training and rehabilitation, mostly based on anecdotal evidence. A review article by Tranquille et al (2017) summarised knowledge from canine and human studies that might be applicable to horses.
They reviewed previous equine studies that had established water treadmill exercise was an aerobic form of exercise, and one that does not appear to induce improvement in aerobic capacity when used within training programmes.

Equine and canine studies have shown water depth can have a significant effect on the biomechanical responses to water treadmill exercise, but the effect of different speeds at the various water depths has not been investigated adequately. They recommended future research should focus on how combinations of water depth and speed alter equine biomechanics compared to overland exercise, determination of long-term benefits of water treadmill exercise, and how to use water treadmill for rehabilitation for horses with specific injuries.
Oral nutraceutical supplements are widely used, with the aim of preventing and managing musculoskeletal conditions, but research into their efficacy is very limited. Murray et al (2017) investigated the effect of an oral supplement (containing chondroitin sulphate, glucosamine, vitamin C, methylsulfonylmethane, docosahexaenoic acid and eicosapentaenoic acid) on limb kinematics, orthopaedic, physiotherapy and handler evaluation in a randomised, blinded, crossover study.
Use of the supplement was associated with decreased lameness score in both straight lines and on the lunge, improved range of motion and muscle tone on physiotherapy examination, and with greater tarsal flexion in horses with hindlimb lameness, determined by high-speed motion capture.
Another US study (Watts et al, 2016) evaluated the effects of oral resveratrol on lameness caused by distal tarsal joint pain in a randomised controlled trial. The study included 45 horses; all received intra-articular triamcinolone in the centrodistal and tarsometatarsal joints, followed by a four-month course of resveratrol or placebo. Complete data were available for 41 horses.
Rider-reported performance measures were significantly better in the supplement than in the placebo group. However, no difference was noted in lameness scores and pelvic movement asymmetry between the supplement and the placebo groups.
It appears our knowledge continues to improve much faster in the diagnosis of injuries than in their treatment and management. In particular, little evidence-based information on rehabilitation techniques is available.
It is hoped an increasing number of studies will be carried out to establish optimal rehabilitation programmes for orthopaedic injuries.