6 Apr 2021
Karin Kruger BVSc, MSc, DipACVIM, MRCVS discusses challenges and changes in the field and hospital regarding horses.
Karin Kruger
Job Title
Image: byrdyak / Adobe Stock
This article will focus on the challenges, changes and innovations in equine anaesthesia and sedation. For details on the principles and procedures of sedation and anaesthesia, you may refer to articles previously published in Vet Times.![]()
This independent article is sponsored and supported online by Chanelle Pharma.
Anaesthesia in horses is a serious business. The Confidential Enquiry into Perioperative Equine Fatalities (CEPEF) 2 was a multicentre prospective observational study with 41,824 cases between 1991-6 that was published in 2002.
The study found an overall death rate of 1.9%, which reduced to 0.9% in healthy patients and increased to 11.7% in colics1. These numbers are significantly higher than in human or small animal anaesthesia.
Due to the significant risks associated with general anaesthesia, many clinicians have developed techniques to perform a variety of surgical and other procedures standing.
More and more procedures of increasing complexity and duration are safely being performed in awake, standing horses.
While short procedures are performed after bolus injection of sedatives and analgesics, longer standing procedures are often performed using a continuous infusion of sedatives, muscle relaxants, dissociative agents and analgesics to facilitate immobility and analgesia.
This is commonly done in hospital settings, but can also be used in the field with a bit of additional planning and equipment, such as portable stocks.

Many examples exist of innovative procedures performed standing in horses. Arthroscopy of a variety of joints can be performed standing, including caudal cervical facet joints2, tarsocrural joints3, temporomandibular joints4, and radiocarpal and middle carpal joints.
Nephrosplenic space ablation and ovariectomy are routinely performed standing. Techniques for replacing a left-displaced colon (nephrosplenic entrapment) and splenectomy via standing flank laparotomy are described5,6. Other standing procedures requiring prolonged sedation include MRI, laparoscopic pneumatic impact lithotripsy for cystoliths, lumbosacral epiduroscopy, fracture repair, tenotomy and a variety of upper airway surgeries7,8.
Recent publications broaden our understanding of how each of the drugs at our disposal perform in different circumstances:
In limited circumstances, sedation and local anaesthesia may be adequate to facilitate noxious procedures in non-standing equids. Donkeys, miniature horses or small ponies, and young foals can often be restrained in lateral recumbency using heavy sedation without the need for general anaesthesia. Gandini et al described a sedated low left flank laparotomy for emergency field caesarean in miniature horses and ponies14.
The most appropriate α2 agonist to choose in the field may depend on the anticipated length of the procedure and the desired recovery time.
In a recent blinded field anaesthesia study, horses were castrated after sedation with either xylazine or detomidine, followed by midazolam and ketamine induction. Horses in the detomidine group had a better plane of surgical anaesthesia and were significantly less likely to require maintenance doses of ketamine. They also took longer to recover, but the quality of induction and recovery did not differ between groups15.
Hypoxaemia is very common and significant in horses anaesthetised without mitigating interventions. This is one of the reasons why many hospital-based equine anaesthetists routinely ventilate their patients. Even in a field situation without a ventilator, supplemental oxygen can be administered via insufflation.
In a field study by Coutu et al, a portable oxygen concentrator delivering pulsed-flow oxygen at 192ml per bolus via nasal insufflation was shown to decrease hypoxaemia. It is worth noting that the horses were still hypoxaemic, but significantly less so than without the supplemental oxygen16.
Another viable option to deliver supplemental oxygen in the field is with a portable oxygen tank and a demand valve (Figure 1).
ooking back at the original CEPEF study, cardiac arrest or cardiovascular collapse caused approximately a third of deaths. A third was caused by fractures and myopathies, and a third was due to abdominal, respiratory or CNS complications, postoperative haemorrhage, acute deaths and other reasons.
Horses maintained on inhalation agents and those that received acepromazine as part of their premedication were significantly less likely to die from cardiac arrest. Patients induced with inhalational agents were almost three times more likely to suffer cardiac arrest1.
A follow-up study looking at 11,336 anaesthetic episodes between 1997-9 (CEPEF3) tried to ascertain whether isoflurane was safer than halothane for inhalation anaesthesia. Although isoflurane reduced the risk associated with cardiac arrest, the risk of other complications increased – particularly those related to the CNS.
Patients that had their blood pressure monitored were significantly less likely to die from cardiac arrest. Operations lasting longer than 90 minutes were 10 times more likely to result in myopathy, and lateral body position increased myopathy risk17.
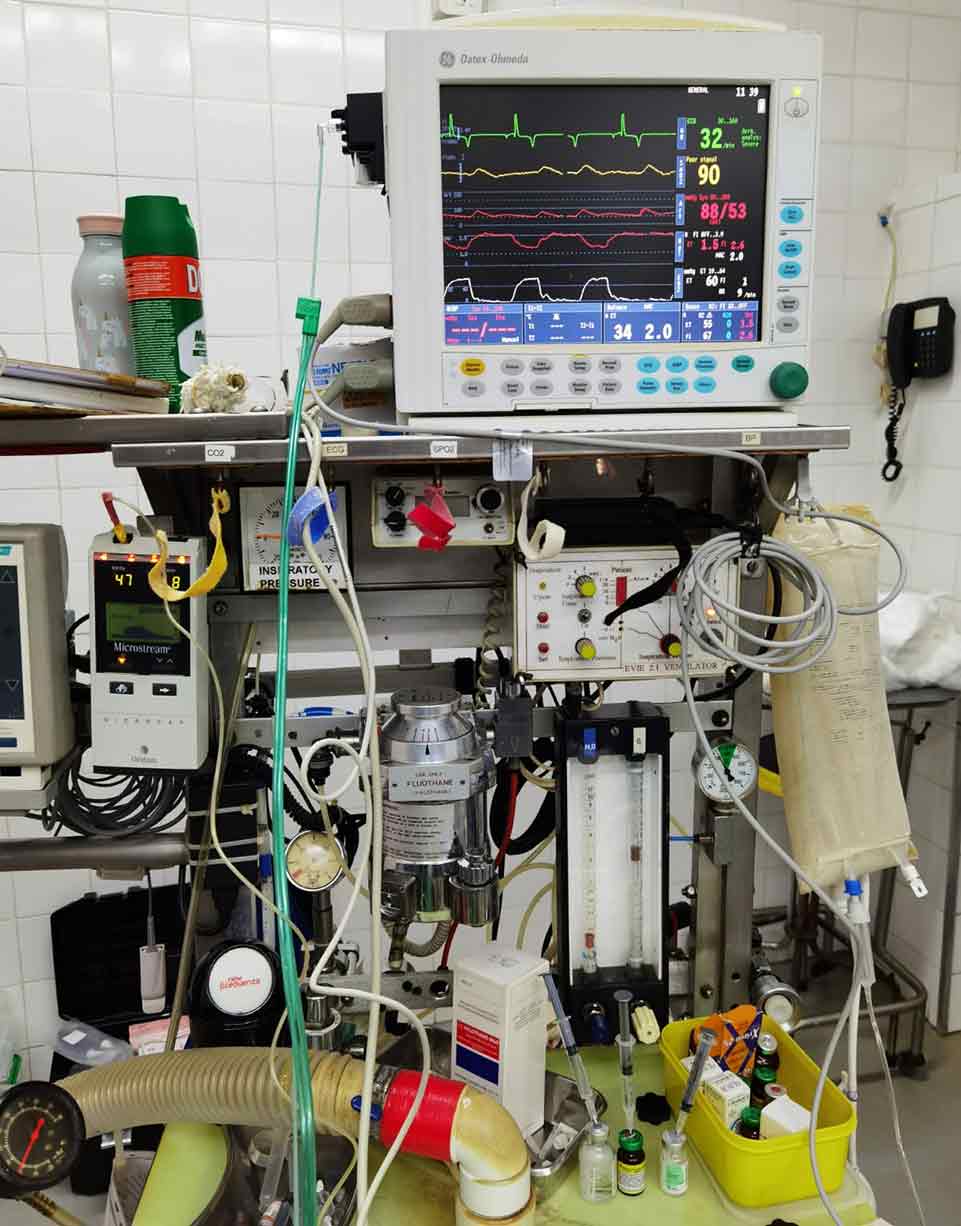
A lot has changed since these studies were performed. Halothane is no longer used, and new drugs and anaesthetic protocols, anaesthetic machines, ventilators, sophisticated monitoring equipment and infusion pumps exist that all improve anaesthetic safety (Figure 2).
Partial IV anaesthesia protocols are used to decrease the minimum alveolar concentration of volatile anaesthetics, which promotes better cardiovascular function (Figure 3). Drugs commonly used for this purpose include α2 agonists, lidocaine, benzodiazepines, ketamine and opioids. In single clinic settings, significantly lower anaesthetic mortality rates compared to the CEPEF studies have been reported, such as the 0.12% fatality rate reported by Bidwell in 200418.
Innovation in equine anaesthesia comes from critically evaluating research findings to devise better anaesthetic protocols, and investing in mechanical ventilators and monitoring equipment that facilitate early appropriate intervention before adverse events occur.
While purpose-designed veterinary monitors exist, human anaesthetic monitors can often be adapted to use in equine patients, which facilitates real‑time monitoring of many critical parameters.
Heart rate, mucous membranes, peripheral perfusion, electrocardiography, pulse oximetry and arterial blood pressure all pertain to cardiovascular function, with arterial blood pressure being the best overall indicator. To maintain adequate microcirculation, anaesthetists should aim for a mean arterial pressure above 70mmHg. By having access to real-time blood pressure monitoring, the anaesthetist can take appropriate remedial action when mean arterial pressure falls below this target.
The pulse pressure (systolic minus diastolic pressure) is another important predictor of the adequacy of perfusion. Appropriate interventions for hypotension could include a reduction in anaesthetic depth; fluid therapy; and cardiovascular stimulant drugs, such as chronotropes, inotropes and vasopressors.

End-tidal CO2 provides an easy way to assess ventilation non-invasively, as it is related to arterial CO2. The best measure of adequacy of ventilation is arterial blood-gas analysis. Several point of care analysers are available that can be used both in the hospital and the field. Detecting hypercapnia and hypoxaemia allows us to take corrective action.
We know that horses suffering from hypoxia during anaesthesia for exploratory laparotomy are significantly more likely to develop incisional infections19. Appropriate interventions could include changing mechanical ventilator settings or tilting the patient slightly (reverse Trendelenburg) to reduce the abdominal organs’ pressure on the diaphragm. In a field setting, emergency ventilation can be achieved using a source of compressed air or oxygen and a demand valve.
Mechanical ventilation should no longer be a last resort for patients that fail to breathe on their own. It is well established that introducing intermittent positive pressure ventilation directly after induction will result in better minute ventilation and arterial oxygenation. This is particularly important if a long procedure is anticipated.
Although equine anaesthetic mortality remains high compared to other species, patient survival sets the bar too low to define a successful outcome. To advance equine anaesthesia, we need to anticipate the risks and take steps to prevent adverse events before they occur.
In aviation and human medicine, this is done through critical incident reporting systems (CIRS) and checklists. In CIRS, all incidents that have the potential to cause harm are recorded and reviewed, and appropriate measures implemented to prevent future occurrences. This is done regardless of whether the incident resulted in an adverse event and has proven effective in decreasing future adverse events.
In 2012, a group of equine anaesthesia experts convened a panel meeting to discuss implementing CIRS in equine anaesthesia20. Examples of preventable critical incidents suggested by the panel include:
In addition to CIRS, surgical safety checklists aim to prevent problems before they occur, and are likely to increase safety and improve outcomes in equine surgery and anaesthesia.
The fourth CEPEF study is under way, and will most certainly lead to further innovation in equine anaesthesia. For those who want to get involved, more information is available on the research group website: https://cepef4.wordpress.com