12 Nov 2018
Safia Barakzai looks at which cases can benefit from the use of this airway assessment technique in equine patients.
Safia Barakzai
Job Title
Figure 1. Endoscopy of a horse at rest.
Exercising endoscopy is sometimes viewed as an expensive extra diagnostic test, but does it give information that is worthwhile and changes the treatment plan? This article discusses which cases exercising endoscopy is particularly useful for.
Resting endoscopic examinations of the nasopharynx and larynx in horses presented for investigation of abnormal respiratory noise and/or poor performance during exercise are performed for two principal reasons – to identify gross structural abnormalities apparent at rest, and to use the appearance and function of the larynx or nasopharynx at rest as predictors for their function during exercise (Figure 1).

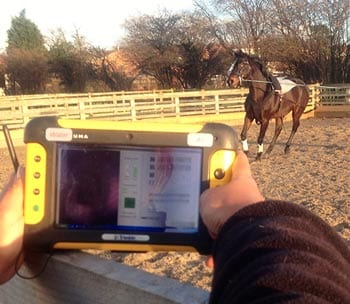
Endoscopic examination of horses running on the treadmill (Figure 2) was the sole method of evaluating the upper respiratory tract at exercise until the late 2000s, when mobile overground endoscopy units (Figure 3) began to be developed.
The past seven to eight years has seen a considerable increase in the availability of these remote overground endoscopic systems. This has made exercising endoscopy accessible to a wider variety of operators and clients, as treadmill examination was restricted to a handful of vet schools and the AHT in the UK.
In the past, it would be fair to say the majority of horses undergoing upper respiratory surgery had a diagnosis made using an educated guess of the most likely pathology present, based on their history and results of resting endoscopy. In some cases, the rider’s influence, changes in head and neck position, track surface or running in company might be key to reproducing the respiratory obstruction.
Overground endoscopy has lent itself to use in situations previously unheard of – such as when horses are showjumping or during Standardbred racing. Theoretically, more targeted treatment of horses that have an accurate diagnosis made using exercising endoscopy should improve surgical success rates.
Essentially, any horse reported to make an abnormal respiratory noise during exercise, and that has either a normal resting scope or is of an equivocal laryngeal grade, is a good candidate for exercising endoscopy. Horses with laryngeal dysplasia also exhibit a wide variety of abnormalities at exercise and are worth investigating further, under exercising conditions.
In the author’s view, even horses with severe laryngeal dysfunction (recurrent laryngeal neuropathy, laryngeal paralysis) should ideally have an exercising endoscopic examination prior to surgery to rule in or out bilateral vocal fold and/or aryepiglottic fold collapse.

Arytenoid function at exercise is graded at A to C using the Havemeyer system, with A being full abduction, B being partial abduction and C being an arytenoid that is held in the cadaveric position, including those that get sucked across the midline during inspiration.
It has been proposed to add an additional grade (D) to differentiate between horses with relatively stable arytenoids that are held in the “cadaveric” position (C) from those that are unstable and collapse further during exercise (D). Vocal fold collapse is also categorised as a form of dynamic laryngeal collapse.
Several grading systems for laryngeal function at rest have previously been described in the literature, and their purpose is to predict how the larynx will behave during exercise.
In 2003, a consensus system of endoscopic laryngeal grading (the Havemeyer system) was developed by an international panel of specialists1. Generally speaking, horses with grade 1, 2.1 and 2.2 laryngeal function are deemed to be within normal limits, and have a fairly low prevalence (3% to 7%2-4) of dynamic laryngeal collapse (vocal fold or arytenoid cartilage collapse).
At the other end of the scale, horses with grade 4 laryngeal function at rest ubiquitously experience complete collapse of the left arytenoid and often bilateral vocal fold collapse and right or bilateral aryepiglottic fold collapse.
Horses with Havemeyer grade 3 laryngeal function, often referred to as the equivocal grade, present the most challenges to clinicians as they can exhibit a wide range of laryngeal appearances during exercise. Choosing an appropriate surgery for these horses should be reliant on the results of exercising endoscopy.
Exercising endoscopy is required to make a definitive diagnosis of palatal dysfunction; however, in the clinical situation, access to such facilities and equipment may be limited, and it can be challenging to persuade some owners and trainers of the value of such examinations. Contradictory evidence exists regarding the usefulness of resting endoscopic findings in predicting the development of dorsal displacement of the soft palate (DDSP) at exercise3,5,6.
Palatal dysfunction at exercise incorporates the syndromes of DDSP and palatal instability (PI)3. While diagnosing DDSP during overground endoscopy is generally clear-cut, diagnosing PI is relatively subjective.
Severe PI has been shown to negatively affect ventilatory parameters in exercising horses and observation of PI is sometimes described as equivalent to a presumptive diagnosis of DDSP. However, not all equine clinicians are in agreement that the two disorders are necessarily linked, because DDSP may occur without being preceded by PI.
It is also unclear what degree of exercise-related soft palate instability can be regarded as normal or physiological, and what percentage of horses diagnosed with PI on high-speed treadmill endoscopy may experience DDSP under different conditions, such as racing.
Although many horses with laryngeal dysplasia can be diagnosed definitively with laryngeal palpation and resting endoscopy, exercising endoscopy is a key diagnostic tool to ascertain which structures are functioning abnormally and obstructing airflow.
This is of great importance when selecting a suitable treatment option and may provide a more accurate prognosis. Dynamic rostral displacement of the palatopharyngeal arch, partial or full arytenoid collapse, left and right vocal cord collapse, and medial deviation of the aryepiglottic fold are all common in these horses.
Several other dynamic disorders exist that can only be observed in the exercising horse, because these horses essentially appear normal during resting endoscopy. These include intermittent epiglottic entrapment, epiglottic retroversion, medial deviation of the aryepiglottic folds, nasopharyngeal collapse and ventroaxial luxation of the corniculate process of the arytenoids, to name a few.
Investigation of ongoing noise after wind surgery should first involve a resting scope to check no obvious undesirable abnormalities are caused by the surgery. However, most horses will require an exercising endoscopic examination to find out which structures are still collapsing under the increased negative pressures associated with exercise.