16 Nov 2015
Andy Durham
Job Title
Figure 4. Seasonal pasture myopathy case being supported due to marked neck weakness causing head swelling.
Most equine myopathy cases are associated with exercise. Non-exertional myopathies are rarely recognised in horses, but include postanaesthetic myopathy, polysaccharide storage myopathy, vitamin E or selenium deficiency, ionophore toxicosis and immune-mediated myositis (such as following Streptococcus equi infection).
Additionally, several reports from different countries (Europe and US) describe a myopathy seen primarily in young, unexercised, turned out horses, often following inclement weather in the autumn. This condition has frequently occurred as an outbreak and often carries a poor prognosis for survival and recovery.
Although recognised as long as 90 years ago, cases appear to be more common in recent years. The condition has been referred to as atypical myopathy or atypical myoglobinuria, although, as we are seeing more cases, the term “atypical” becomes nonsensical and perhaps a more appropriate and descriptive term now is “seasonal pasture myopathy”.
Multiple cases are frequently reported on the same premises, which has suggested an infectious, toxic or nutritional aetiology. Association with trees in the acer genus (maple and sycamore) has long been recognised and the cause of the myopathy has now been securely identified as ingestion of the toxin hypoglycin A, contained in seeds and seedlings of acer trees.

Around 125 species are recognised worldwide although, excepting gardens and arboretums, only three species are seen in reasonable numbers in the UK, comprising the sycamore (Acer pseudoplatanus), field maple (Acer campestre) and Norway maple (Acer platanoides). Of these three species, hypoglycin A has only been identified in the sycamore (Figure 1) although, given relatively limited research in this area and the known variability in toxin production, it is hard to fully rule out the possible presence of hypoglycin in other species of tree.
Studies have identified hypoglycin in several non-native species also, comprising Acer japonicum, Acer macrophyllum, Acer negundo, Acer palmatum, Acer saccharinum and Acer saccharum.
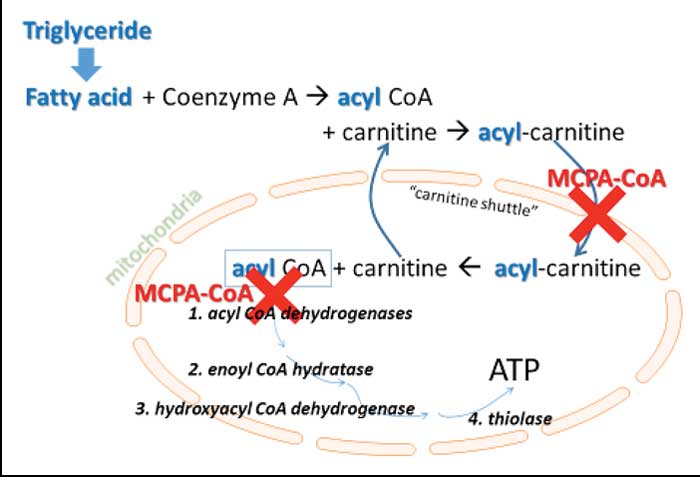
Ingested hypoglycin A is biotransformed to methylene-cyclopropyl-acetic acid (MCPA), which binds coenzyme A to form MCPA-CoA, which, in turn, causes multiple acyl-CoA dehydrogenase deficiency, with the effect of blocking mitochondrial fatty acid oxidation in type-one (oxidative) muscle cells (Figure 2).
Fatty acids are the major fuel of these cells and hence adenosine triphosphate production is greatly limited, in addition to the build-up of toxic intermediates. Muscles rich in type-one fibres are generally postural and respiratory muscles rather than those associated with power and ambulation and this is reflected in the clinical signs.
Affected cases generally demonstrate sudden onset of weakness and stiffness, perhaps with tremors and sweating, which may then progress to recumbency. Cases can sometimes be managed while recumbent, although supportive slings are helpful (Figure 3).
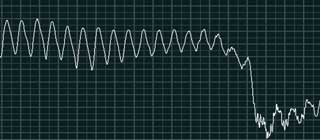
Myoglobinuria is frequently observed. Profound neck weakness with low head carriage and head oedema is sometimes seen (Figure 4). Some cases may be found dead with no previously observed clinical signs. Pyrexia is uncommon and appetite is variable. Tachycardia is common and occasionally arrhythmias may be detected (Figure 5). Respiratory distress is a poor prognostic sign and probably reflects intercostal muscle and diaphragm damage. Apparent head-tossing behaviour, mild diarrhoea and choke may sometimes also be seen.



Deterioration over 24 to 48 hours is common, even after removal from pasture, perhaps due to the time required for toxin biotransformation and pathologic effects. Progression to death may occur in 80% to 90% of cases over the course of 48 to 72 hours, although reported mortality rates of clinical cases have ranged from 33% to 100% and may vary from year to year.
This author’s experience in seeing cases virtually every year since 1991 has indicated the majority of cases do not survive, although in 2011 around 70% of cases admitted to the Liphook Equine Hospital were discharged alive. Most cases still alive at five days are likely to recover, although some have survived as long as a week before succumbing. In cases that have survived, recovery has sometimes been slow and incomplete.
The number of affected animals in outbreaks has been variable. Single cases are reported, although it is common for two or more to occur on the same premises within a few days of each other. One outbreak in Germany resulted in the death of 111 out of 115 horses.
Where single clinical cases are seen, blood testing often reveals many subclinically affected herd mates. Recurrence on the same premises in subsequent years has been reported.
Seasonal pasture myopathy is easily missed as a diagnosis. Many cases may appear to be affected by colic and it is by no means unheard of for cases to be subject to exploratory laparotomy before the actual diagnosis is reached.
In terms of clinical examination (or postmortem examination), it is often the urine that gives the diagnosis. If pigmenturia (myoglobinuria) is noted then the diagnosis becomes more obvious. Urinary dipsticks will reveal myoglobinuria (“blood-positive”) where pigmenturia is not grossly obvious, and glycosuria is also common.
Measurement of serum or plasma creatine kinase (CK) reveals rapidly increasing levels, but has no prognostic relevance. Prompt sampling might not reveal very high CK levels, but further increases within four to six hours will then be seen.
Cardiac troponin I may be increased in some cases, reflecting cardiac myopathy. Low arterial oxygen and high lactate levels may be useful prognostic indicators reflecting poor respiratory function and perfusion. Hyperglycaemia, hypertriglyceridaemia and hypocalcaemia are also very commonly seen. In addition to myopathy, there is often biochemical evidence of hepatopathy.
Muscle abnormalities are not always obvious at postmortem, although pallor and haemorrhage is reported in some cases, especially in intercostals, diaphragm, neck and shoulder muscles, as well as occasional cardiac involvement. Myoglobinuria may be detected on examination of the bladder. Histopathologic changes are found in type-one rather than type-two muscle fibres. They are most consistently found in the diaphragm and intercostal muscles. Oil red O staining indicates marked lipid accumulation within myocytes.
Treatment for suspected cases of seasonal pasture myopathy is largely supportive. Many cases show extreme pain that is unresponsive to analgesics and probably warrant euthanasia. Cases showing just stiffness, somnolence and weakness, and less severe pain are more likely to survive. NSAIDs may not be ideal where dehydration and nephrotoxic myoglobin is also causing renal insult. Lidocaine infusion can often be a useful means of providing some analgesia without recourse to NSAIDs, as can alpha-2 agonists, opioids or gabapentin.
Fluid therapy (preferably IV) is essential to provide routine hydration, to protect the kidneys from myoglobin, and to facilitate correction of electrolyte abnormalities.
Initially, high fluid rates of around 10ml/kg/hour to 20ml/kg/hour (5L/hr to 10L/hr for 500kg) should be gradually reduced as the urine clears of myoglobin.
Intranasal oxygen may help tachypnoeic or dyspnoeic cases having difficulty breathing, especially if PaO2 is found to be low. Glucose/dextrose addition to IV fluids has been advocated in view of the finding of lipid accumulation in myocytes, as a possible means of stimulating carbohydrate metabolism, although this has not been critically evaluated.
Given most cases are already hyperglycaemic and hyperinsulinaemic, presumably as a consequence of high circulating catecholamines, this approach appears hard to rationalise and has no evidential support.
Attempts at cardiac stabilisation might be appropriate when arrhythmias are present, although the severity of cardiac muscle damage often leads to disappointing responses. This author has frequently used intravenous lidocaine (10ml to 20ml boluses of 2% solution) and magnesium sulphate (10ml boluses of 20% solution), but with limited success.
Some evidence suggests improved survival with multivitamin administration. Vitamin E requirements should be ensured (>1.0IU [0.7mg] per kg per day) and vitamin C might also be a useful antioxidant. Supplementation with carnitine, vitamin B1 and B2 might also support mitochondrial function.
No breed predisposition has been demonstrated, although unworked young horses and females turned out to pasture are most commonly affected.
The majority of affected cases are younger than four years, but any age may be affected. The high incidence of the condition in young horses may be as a consequence of a primary age susceptibility, different ingestive behaviour or the fact young horses may be more likely to be turned out.
The apparent predisposition in females may result from them being more likely to be turned out also (for example, broodmares) in comparison with stallions and geldings. Additionally, horses in poor body condition that have not received regular prophylactic health care (vaccines and deworming) may be predisposed.
Fields with access to a river, stream or pond, sloping pasture and the presence of dead leaves have all been recognised frequently in outbreaks. Presence of maples and sycamores are common in affected fields, although not all outbreaks have trees that are close.
A strong seasonal incidence is apparent. About 75% of reported cases have occurred in the autumn with the majority of remaining cases occurring in spring, with a few in the winter. Summer cases are rare although a fatal case was admitted by the author in June 2015.
Weather has generally been severe leading up to outbreaks, including cold, cloudy, strong winds, increased humidity, rain and sometimes frosts. Stormy weather most probably increases seed fall and also might encourage the dropping of immature seeds, which might contain more toxin.
Autumnal outbreaks are often followed by further problems the following spring, warranting planned management changes.
Housing horses (especially younger stock not in work), for at least part of the day, in the autumn during and after inclement weather may reduce the incidence of cases. Cases are extremely rare in horses grazing for less than six hours per day. Where this is impractical then forage should be provided, perhaps in association with restricting the turnout area and fencing off areas near trees with dead leaves/seeds on the ground.
Tap water should be provided rather than access to natural water sources. Access to a salt/mineral block may be helpful along with general health care including regular vaccination and deworming.
When a case is seen or suspected then herd mates should be removed from the pasture and CK measured, as subclinical cases are common. Provision of multivitamin supplements may be worthwhile.
Seasonal pasture myopathy is a very distressing disease causing severe and frequently uncontrollable pain in affected horses.
The associated poor prognosis creates significant dilemmas for the attending veterinary surgeon who must judge whether euthanasia or attempted treatment is the best option. The disease should always be considered when cases of sudden death or severely ill horses are encountered in the autumn. Definitive clinical or postmortem signs of muscular disease are not always obvious, but urine will generally be discoloured as a supportive indicator of myolysis.