4 Feb 2020
Nicola Menzies-Gow MA, VetMB, PhD, DipECEIM, CertEM(IntMed), FHEA, MRCVS discusses how feeding an appropriate diet can help prevent a number of common diseases in horses and ponies.
Nicola Menzies-Gow
Job Title
Nutrition plays an important role in managing and preventing a number of equine diseases.
In equine metabolic syndrome, nutritional strategies are employed to reduce obesity in animals with generalised or regional adiposity, and minimise the postprandial insulinaemic response in both obese and lean animals.
Animals with pituitary pars intermedia dysfunction (PPID) may be ideal body condition, underweight or overweight. In addition, a subset of animals with PPID have insulin dysregulation (ID). Therefore, feed selection should be based on body condition score and evidence of ID.
Equine gastric ulcer syndrome encompasses equine squamous gastric disease (ESGD) and equine glandular gastric disease (EGGD).
Animals with ESGD should, ideally, have continuous access to good-quality grass pasture. Alternatively, free choice – or at least frequent feedings (four to six meals per day) – of forage may be a suitable replacement. Grain and concentrates should be fed as sparingly as possible, divided into at least three meals per day, and water provided continuously.
Limited evidence exists on which to make recommendations for feeding horses with EGGD; however, it would seem logical to maximise grazing and ensure exercise is not performed on an empty stomach. Additionally, inclusion of oils – such as corn oil, maize oil or rapeseed oil – and mucosal protectants, such as pectin or lecithin, in the diet may be of benefit.
Nutrition plays an important role in the management and prevention of a number of equine diseases.
This article will focus on four of the more common diseases:
EMS is a collection of risk factors for endocrinopathic laminitis.
The key central and consistent feature of EMS is insulin dysregulation (ID), which may manifest as hyperinsulinaemia, an excessive insulin response to oral carbohydrate and/or tissue insulin resistance.

Additional features include obesity, hypertriglyceridaemia and altered circulating concentrations of adipokines.
Management of EMS focuses on nutritional strategies to manage obesity in animals that have generalised (Figure 1) or regional adiposity, and exercise to improve insulin sensitivity once any laminitis has resolved.
Pharmacological aids, such as metformin and thyroxine, can be used in the short term in animals that are resistant to dietary management and exercise alone.
Obesity is managed primarily via energy restriction through limiting intake.
An ideal target for weight loss is 0.5% to 1% of body mass (BM) weekly. To achieve this, a daily allowance of between 1.25% and 1.5% of actual BM as dry matter intake (DMI) – or between 1.4% and 1.7% of actual BM as fed – is widely recommended.
In horses with weight loss resistance, a further forage restriction to 1.0% BM as DMI – or 1.15% BM as fed – may be considered if appropriately monitored.
The nutrient composition of the forage should be determined where possible and hays with low non-structural carbohydrate (NSC) content (lower than 10%) are recommended to limit postprandial insulin responses.
Soaking is advised to reduce the NSC content of the hay, if necessary, and as forages can be low in protein – and mineral and vitamin leaching occurs after soaking – these nutrients must be balanced by low-calorie supplements to cover requirements.
Due to the greater insulinaemic response provoked compared to a hay with equivalent NSC content and increased palatability, the feeding of haylage is not recommended.
Grains or cereal-based feeds should be excluded due to their high NSC content, while high-fat feeds should be avoided due to their high energy content.
Additionally, large quantities of fruit or vegetables – such as carrots, apples or treats with a high glycaemic load – should be avoided.
During the initial 6 to 12 weeks of dietary restriction, pasture access should be prevented as even partial access is very difficult to quantify. However, successful long-term management of EMS cases can still include some grazing, providing ID – especially assessed by the insulin response to oral carbohydrates or grazing – is under control and grazing is carefully controlled.

The use of dietary supplements – such as cinnamon, magnesium and chromium – to facilitate weight loss or improve ID is popular, but their efficacy remains questionable or unproven.
Bodyweight should be reassessed every 30 days, using a weight scale or weight tape, and dietary adjustments made based on weight loss.
Lean animals with EMS should be maintained on a low glycaemic diet, with the severity of restriction dependent on the postprandial insulin response. The diet should be based on forage with a low NSC (lower than 10%) content and additional calories, if required, should be provided in the form of high-quality fibre content, such as beet pulp, soy hulls or oil.
A mineral/vitamin/protein ration balancer should also be provided.
PPID is a slowly progressive neurodegenerative disease of the horse with loss of dopaminergic (inhibitory) input to the melanotrophs of the pituitary pars intermedia, which appears to be associated with localised oxidative stress and abnormal protein (α-synuclein) accumulation. However, the exact cause remains unknown.
The consequent dysfunction of this region results in hyperplasia of this area of the gland and overproduction of pars intermedia-derived hormones; eventually, the area undergoes adenomatous change.
The clinical signs associated with PPID can be roughly divided into those seen early in the disease and those associated with advanced disease.
Early signs include decreased athletic performance, change in attitude/lethargy, delayed haircoat shedding, regional hypertrichosis (Figure 2), change in body conformation, regional adiposity and laminitis.
Late signs include lethargy, generalised hypertrichosis, skeletal muscle atrophy, hyperhidrosis, polyuria/polydipsia, recurrent infections, infertility and laminitis.
PPID is a slowly progressive, lifelong condition. The aim of treatment is not to cure the condition, but increase the quality of life through reducing the clinical signs, including those that have the potential to be life-threatening.
Pergolide is available as a product licensed in the UK for the treatment of PPID in horses. It is a dopamine agonist, so replaces the lost dopaminergic inhibition to the pars intermedia, reducing hormone production.
Animals with PPID may be ideal body condition, underweight or overweight. Additionally, a subset of animals with PPID have ID; therefore, feed selection should be based on body condition score (BCS) and evidence of ID.
Some PPID horses are lean and have normal insulin status. Senior feeds and pasture grazing are appropriate in these cases.
For obese horses (BCS greater than or equal to 7/9) with PPID, the obesity is managed primarily via energy restriction through limiting intake (see obese EMS animals) and an exercise programme started.
For PPID horses with ID, a diet low in NSC and limited access to pasture is required.
It should be remembered the feed requirements of aged horses – especially those with PPID – may change over time and monthly monitoring of BCS by owners is recommended.
Dietary supplements have been suggested for the management of PPID, but, to date, scientific evidence for their efficacy is lacking.
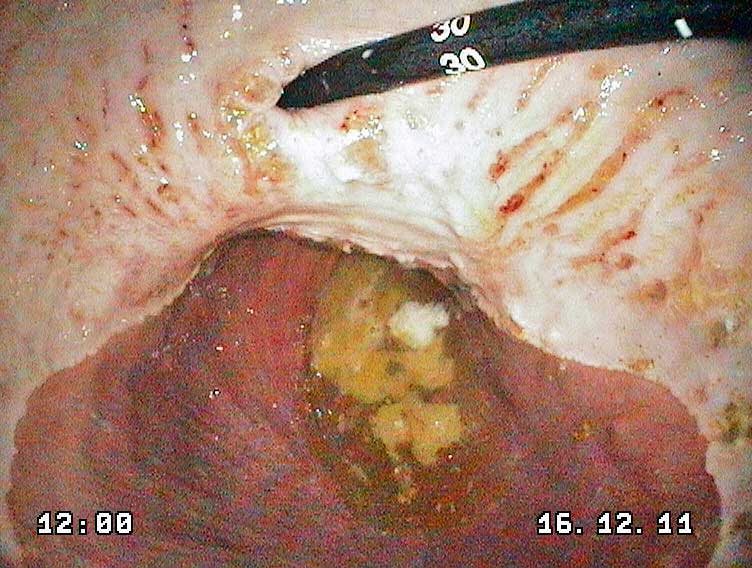
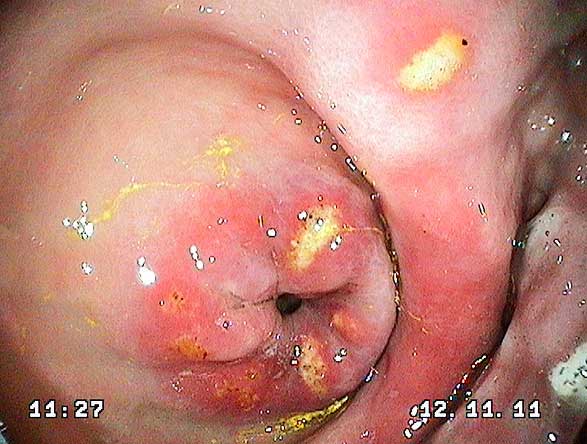
EGUS encompasses equine squamous gastric disease (ESGD; Figure 3) and equine glandular gastric disease (EGGD; Figure 4), which are terms that describe the affected region anatomically.
They differ with respect to their epidemiology, prevalence, risk factors, pathophysiology and response to treatment.
Within ESGD, both primary and secondary disease are recognised. Primary ESGD, the more common of the two forms, occurs in animals with an otherwise normal gastrointestinal tract. In contrast, secondary ESGD occurs in animals with delayed gastric outflow secondary to an underlying abnormality, such as pyloric stenosis.
Although the evidence supporting such a recommendation is conflicting, continuous access to good-quality grass pasture is considered ideal.
Free choice – or at least frequent feedings (four to six meals per day) – of hay may be a suitable replacement, with animals being fed a minimum of 1.5% of actual BM as DMI, or 1.7% of actual BM as fed, per day.
No difference exists between hay (dry, soaked or steamed) and haylage as a forage source in relation to ulceration.
Overweight horses and ponies at risk of EGUS should receive a similar amount of forage with a low (lower than 10%) NSC content. If low-energy forage is not available, a mixture of high-quality forage and straw divided into a minimum of four feedings may be a suitable alternative.
Straw should not be the only forage provided, but can be safely included in the ration at less than 0.25% of actual BM as DMI.
Horses should be fed grain and concentrates as sparingly as possible. Feeding of sweet feed should be avoided, as a large quantity of volatile fatty acids (VFAs) could be produced if more than 1kg to 2kg of sweet feed is fed per meal.
Grains, such as barley and oats, should be substituted to decrease fermentation to VFAs. The diet should not exceed 2g/kg bodyweight of starch intake per day, or more than 1g/kg bodyweight of starch per meal.
Concentrates should be divided into at least three meals per day.
Water should be provided continuously. An increased risk of ESGD has been shown with electrolyte pastes or hypertonic solutions given orally, but not when electrolytes were mixed in feed or given in lower doses in water; as such, electrolytes fed with feed are considered safe.
Limited evidence exists on which to make recommendations for feeding horses with EGGD; however, it would seem logical to maximise grazing and ensure exercise is not performed on an empty stomach – for example, feed two litres of chaff, or an equivalent volume of forage, 30 minutes prior to exercise.
In horses with a history of EGGD, or those considered to be at high risk, vegetable oils – such as corn oil, maize oil or rapeseed oil – (0.1ml/kg BM) may help reduce the risk of EGGD.
Supplemental pectin and lecithin complexes have shown to be of benefit in small numbers of horses; sugar beet is high in pectin and is a less expensive alternative to proprietary pectin and lecithin products, although no data exist to support its use in this setting.
Exertional rhabdomyolysis (ER) is a clinical syndrome in horses characterised by muscle cell damage, pain, stiffness and cramping with exercise.
RER is a specific form of ER – described in Thoroughbreds, standardbreds and Arabs – in which individuals have more than one clinical episode of ER while competing at an appropriate fitness level.
A number of studies have identified risk factors contributing to RER. In Thoroughbred and standardbred racehorses, epidemiological studies have concluded diet, exercise, sex, age and stress are risk factors for development of clinical disease.
It is believed to have a genetic basis and involve an abnormality in intracellular calcium regulation in skeletal muscles.
Prevention of further episodes of RER in susceptible horses should include standardised daily routines and an environment that minimises excitement and stress.
Management changes that may decrease excitement include minimising stable confinement by using turnout or a horse walker, exercising and feeding horses with RER before other horses, and providing compatible equine company.
A nutritionally balanced diet with appropriate caloric intake, and adequate vitamins and minerals, is vital. Hay should be fed at between 1.5% and 2% BM, and the diet should include a balanced vitamin and mineral supplement.
Increasing dietary fat supplementation and decreasing dietary starch have resulted in beneficial effects in horses with RER when total dietary caloric intake is high.
The mechanism for this is not clearly understood, but appears to be related to the exclusion of dietary starch rather than specific protective effects of high dietary fat. In these instances, a high-fat (20% to 25% of digestible energy as fat), low-starch diet (lower than or equal to 20% of daily digestible energy as NSC) is recommended.
If the intensity of the exercise training being undertaken requires a higher caloric intake than can be provided through the addition of vegetable oil or rice barn, specialised feeds designed for ER are necessary.
Some drugs mentioned in this article are used under the cascade.