6 Mar 2017
Emma King looks at key viral, bacterial and fungal diseases found in ducks and how to identify them at postmortem.
Emma King
Job Title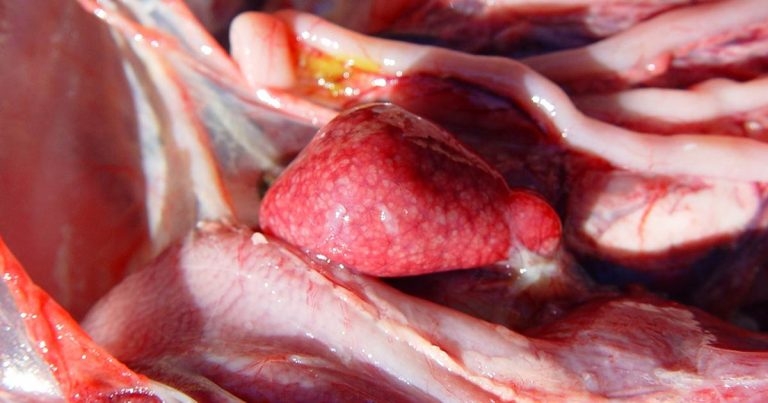
Figure 5. Enlarged, mottled spleen. Image: © Prof JL Guerin, University of Toulouse.
Commercial production of duck meat is a growing industry, in the UK and around the world. The change towards more intensive systems means biosecurity and disease control are becoming more important. Discussed in this article are the clinical signs, diagnosis and treatment of key infectious diseases in the UK, including duck viral hepatitis, duck viral enteritis, Riemerella anatipestifer, Streptococcus and aspergillosis. The notifiable diseases, avian influenza and Newcastle disease, are also briefly described. The focus is given to Pekin ducks, which make up the majority of the UK meat duck population.
The duck meat industry is expanding and changing, both globally and in the UK. There is movement away from the traditional extensive free-range production, towards intensification, environmental control and better biosecurity.
Duck meat production has its own unique challenges, in comparison with other intensively reared poultry species.

The aquatic nature of ducks means maintaining a dry environment is very difficult. It is necessary to re-bed the birds daily with fresh straw, which makes maintaining biosecurity highly problematic. Ducks are also very resistant to disease, which, while having some obvious benefits, also means they can be asymptomatic carriers of diseases, such as avian influenza.
The two most commonly farmed duck species are Pekin (Anas platyrhynchos) and Muscovy (Cairina moschata). Muscovy ducks are more commonly found in France, as they are frequently used in production of foie gras.
This article will focus primarily on Pekin ducks, as these birds make up the vast majority of the UK duck grower population. Important viral, bacterial and fungal diseases are discussed in this article.
Two main viral diseases are specific to ducks in the UK. The first is duck viral hepatitis (DVH). Three antigenically different viruses have been identified associated with DVH and the disease is classed as types 1 to 3.
Type 1 naturally infects ducks only, and is the most widespread and most virulent. It is an acute, highly infectious disease of ducklings, primarily affecting birds up to three weeks old. Immunity is slowly built with age, with negligible mortality from four to five weeks onwards1.
Once confirmed on site, type 1 can remain viable in the environment for weeks to months. Rapid spread will take place within a flock to all susceptible birds1 and the key routes of transmission are faecal-oral or by fomite, such as contaminated equipment, vehicles and staff. Vertical transmission does not occur2.
DVH type 1 typically presents acutely or per-acutely, with affected birds frequently in good body condition.
Mortality can be more than 90% if virus is introduced into a young naïve flock1 and is generally 5% to 10% in an endemic situation. Sudden death is the most common clinical sign, but ducklings can also show opisthotonus (Figure 1). Signs that can be seen on postmortem examination are hepatomegaly with petechial/ecchymotic haemorrhages1 (Figures 2 and 3), secondary bacterial septicaemia (common in older birds) and fatty kidneys3. Definitive diagnosis is by virus isolation (such as by inoculation of blood or organ material into the allantoic sac of an embryonated egg)4, direct immunofluorescence of the liver, or PCR5.


A serological test is available, but it is uneconomical on a commercial scale.
Control of DVH relies on vaccination, normally of the breeder flock, with one live primer, followed by one inactivated vaccine. Good hygiene and biosecurity, and thorough disinfection between flocks, are also key, due to the resistant nature of this virus once it is present in the environment.
One of the important differential diagnoses for DVH, and the second duck-specific viral disease, is duck viral enteritis (DVE). DVE, also known as “duck plague”, was first diagnosed in the UK in 19726. Outbreaks in commercial birds are often associated with access to natural water and swimming sources, and contact with wild waterfowl7.
DVE is one disease with a difference in susceptibility between duck species. Muscovy ducks are more susceptible and, if the flock is mixed, will often be the first to show clinical signs and mortality. Pekin ducks are more resistant and wild species, such as mallards, even more so8.
Regarding transmission, water is a risk factor, as both the oral and cloacal routes are sources of infection. DVE is a herpesvirus and so, once infected, the virus can remain latent in the trigeminal ganglion of immune carrier birds and be shed periodically9.
Like DVH, DVE commonly presents acutely. Clinical signs include ataxia (wings used to support walking or swimming), nasal and ocular discharge, photophobia and blood-stained vents as a sequelae of watery, haemorrhagic diarrhoea10. Again, postmortem examination can be useful in diagnosis.
DVE is a vascular disease and, as such, can lead to haemorrhage in multiple organs (including, but not limited to, the heart, pancreas, liver, kidneys and lungs), and free blood in the body cavity. Haemorrhages can also be found on the mucosal surface of the GI tract, particularly the oesophagus, and this can progress to necrotic foci in the later stages of the disease. Necrotic foci may also be found in the liver.
Other than postmortem, the other key diagnostic tool is PCR11 – again, a routine serological test is not readily available.
As with DVH, control of DVE relies on effective biosecurity and good hygiene. Clear separation from wild birds is particularly important. A live attenuated vaccine is available in other countries, which has been shown to be more effective than inactivated vaccines12.
Two viral diseases affecting ducks that are notifiable in the UK are avian influenza and Newcastle disease.
Avian influenza presents slightly differently in ducks, in comparison with chickens and turkeys. Mortality and respiratory clinical signs are often much less severe and, frequently, are entirely absent, even when infection is with a highly pathogenic strain. Often the only indicator of disease presence is a drop in egg production. Regardless, ducks are still of significant importance as a vector for the spread of the virus – they are capable of shedding 108.7 infectious virus particles per gram of faeces13.
Newcastle disease is caused by type 1 paramyxovirus. The disease can present in four forms – viscerotropic, neurotropic, mesogenic and lentogenic – which means clinical signs can be very varied, and may include depression, diarrhoea, prostration, oedema of the head and wattles, and nervous and respiratory signs14.
Newcastle disease is highly virulent in chickens, but ducks, again, show a much greater degree of resistance and a common presenting sign is a decrease in egg production.
The majority of bacterial diseases in ducks are associated with poor hygiene and biosecurity. As with the other commercial poultry species, Escherichia coli, Pasteurella and Salmonella enterica (particularly Typhimurium sub-species) are major bacterial pathogens.
For practicality, only two bacteria are discussed here in depth – Riemerella anatipestifer and Streptococcus, which generally affect ducks, in particular.
R anatipestifer is a Gram-negative, non-motile rod, which causes systemic infection, particularly in young birds. Ducklings up to eight weeks of age are highly susceptible, and birds infected at less than five weeks old usually die within one to two days if left untreated15.
R anatipestifer survives in the environment, and can reportedly persist for up to 39 days in litter16. Infection takes place through the respiratory tract, or through skin wounds, particularly on the feet. The severity of disease seen depends on the route of entry, with more severe signs seen with IV infection (through wounds, for example) than with the oro-nasal route17.
The incubation period of the bacteria is two to five days and a high morbidity is usually seen.

Mortality can vary, based on factors such as age, stocking density and concurrent pathogens, and has been reported between 5% and 75%. The clinical signs seen are commonly depression, ocular and nasal discharge, mild coughing and sneezing, greenish diarrhoea, and neurological signs, including ataxia, and head and neck tremors. The growth of surviving ducklings may be stunted18.
At postmortem, the clearest gross lesion is a fibrinous exudate covering serosal surfaces, particularly producing pericarditis, perihepatitis and air sacculitis (Figure 4). The spleen may also be mottled and enlarged. However, both of these lesions are inspecific and bacterial culture is required for definitive diagnosis.
Swabs for culture may be taken from various tissues, including the brain, heart blood, air sacs, bone marrow, lungs and liver.
Some strains of Riemerella are particularly fastidious and difficult to culture. The recommended medium is chocolate or blood agar, with additions of 0.05% yeast extract and 5% newborn calf serum. However, depending on the laboratory facilities available, sending samples to a specialist laboratory is recommended.
Aside from culture, other possible diagnostic methods are immunofluorescence19 or PCR of affected tissues, such as the lungs.
Treatment of R anatipestifer is by antibiotic therapy, based on bacterial sensitivity. The most commonly used antibiotic in duck production in the UK is amoxicillin, which is licensed and generally produces a good response. Vaccination is also an option, with both live and inactivated bacterin vaccines licensed in other countries. Live vaccines can be given to breeder flocks, with maternally derived antibody shown to give protection up to two to three weeks of age, or to day-old ducklings via water or aerosol spray20. However, for long-term management of R anatipestifer, neither vaccination or antibiotic therapy is a substitute for improvements in basic hygiene, and in cleaning and disinfection protocols at turnaround.

A second bacteria that causes particular problems in ducks is Streptococcus. Streptococci are Gram-positive, non-motile bacteria, which form part of the normal intestinal and mucosal flora. As with other commensal bacteria, such as E coli, it is suspected their overgrowth into pathogenic significance is secondary to a greater underlying problem. Streptococcus infection in ducks typically affects young birds, frequently presenting as sudden death in ducklings – particularly up to three weeks old21. Often, few other clinical signs will be seen, although neurological signs, such as tremors, fitting and opisthotonus, have been reported22.
At postmortem, lesions seen are non-specific. The most common findings are hepatomegaly and splenomegaly, with additional mottling of the spleen (Figure 5). As with Riemerella, culture is required for definitive diagnosis. Swabs can be taken from the liver, spleen or heart blood and Streptococcus is generally easily grown on blood agar23. The most common septicaemia-causing species isolated in ducks are Streptococcus bovis or Streptococcus gallolyticus24.
Treatment for Streptococcus is, again, based on antibiotic therapy. This should be based on bacterial sensitivity as far as possible, but licensed options are limited in the UK. Amoxicillin is licensed, and oxytetracycline is licensed in other countries, and can be imported. As with R anatipestifer, in the long term, improved hygiene and management are necessary to reduce environmental reservoirs of Streptococcus to a minimum23.
Fungal infection is of greater importance in ducks than in other commercial poultry species. The main cause of this is the reliance on straw as a bedding substrate. Poor quality or mouldy bedding can often contain high numbers of fungal spores25.
Aspergillus is the main fungus, with Aspergillus fumigatus the most common species isolated26.
Aspergillosis is not infectious between birds – exposure to environmental sources, including in ovo27, are the only route of infection26.
Aspergillosis can present in an acute or chronic form. In grower ducks, the acute form is more common, with respiratory signs, such as dyspnoea and gasping, and depression and mortality seen. This is the most common presentation, as lesions are usually confined to the lower respiratory system, in the air sacs and lungs. However, there are more unusual forms of the disease, with lesions in the eye28, brain29, bone30 and other viscera. The chronic form of aspergillosis is more common in breeder ducks, with their longer lifespan. Aspergillosis, in general, is also more significant where other stress factors are involved.

Confirmation of aspergillosis is usually by postmortem, followed up by histology or culture. The lesions that can be seen at postmortem are white miliary foci on the air sacs and white caseous nodules throughout the lungs. As the disease advances, air sacs will become progressively thickened and opaque, and the white foci can coalesce into granulomas26 (Figure 6). Histology of a section of lung or air sac can then be used to confirm the presence of the fungus, as can culture of a small piece of either of these tissues. A special culture medium is required – sabouraud dextrose26 or rose bengal agars both work well.
No licensed antifungals exist for ducks and no effective vaccines. Control of Aspergillus relies on environmental management, centring especially around the straw bedding. Straw bales should not be used if they appear mouldy – if there is concern over quality, then a fungal spore count can be performed. If there is an outbreak of Aspergillus in a shed, then it is wise to re-bed with clean straw as soon as possible. Particular attention should also be paid to feed quality and hygiene at hatchery. In conclusion, while susceptible to a range of infectious diseases, ducks are impressively resistant birds. While this has a positive side, it also means the role of waterfowl as reservoir hosts should always be an important consideration.
As with disease control across all species, good biosecurity plays a vital role. Despite the biosecurity challenges associated with duck rearing, it is particularly important for these birds, given the comparatively limited
range of licensed antibiotics and vaccines available in the UK.