18 Apr 2016
Helen Sumner describes the diagnosis and treatment of a young female dog with renal failure and the efforts of a veterinary team to give her some quality of life.
Helen Sumner
Job Title
Figure 1. Bailey had presented with a history of inappetence, polydipsia and occasional vomiting.
Renal disease is commonly seen in older animals, but less frequently encountered in juvenile patients in general practice. This article follows the case of a boxer dog diagnosed with renal failure at 11 months of age and includes its presenting signs, diagnostic investigations and treatments used to manage the condition. Management of non-regenerative anaemia with synthetic erythropoietin analogue darbopoietin was an important part of the treatment regime. The possible causes of renal disease in young dogs are discussed, along with the similarities and differences found in a variety of dog breeds. Renal disease in young boxers has been compared in several studies to juvenile human kidney conditions involving reflux nephropathy as a cause of renal damage.
In general practice, we are all familiar with renal disease in older patients, with one study suggesting more than 20% of dogs more than five years of age have reduced renal function1; however, it is much more unusual to see this in younger animals.

When presented with Bailey (Figure 1), an 11-month-old female entire boxer with a history of inappetence, polydipsia and occasional vomiting, we were surprised to find a marked azotaemia.
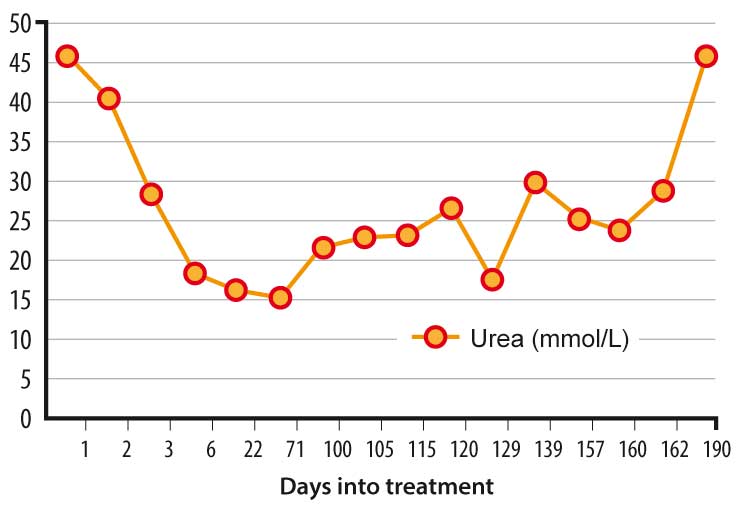
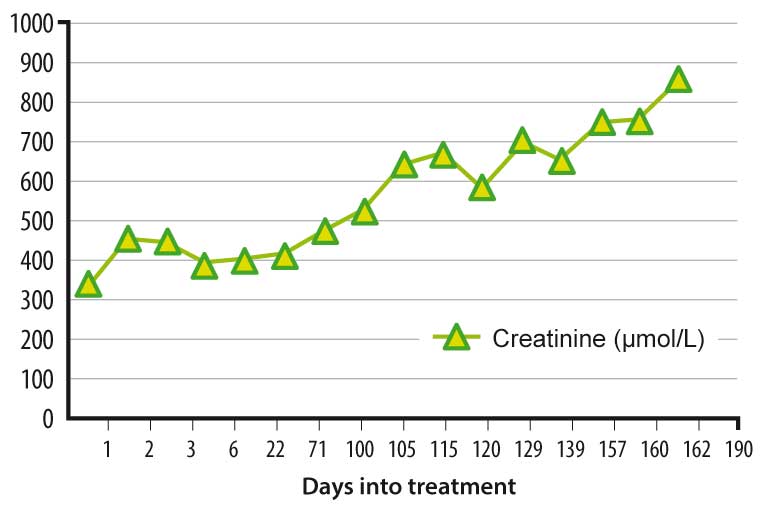
A general biochemistry and haematology profile revealed a blood urea of >46mmol/L (normal range 2.5mmol/L to 9.6mmol/L) and creatinine 342µmol/L (normal range 44µmol/L to 159µmol/L).
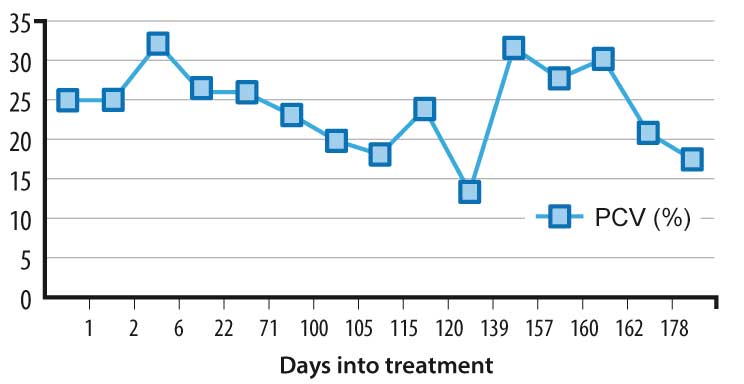
In addition to this, she was hyperphosphataemic at 3.09mmol/L (normal range 0.81mmol/L to 2.19mmol/L) and moderately anaemic, with a PCV of 25% (normal range 37% to 55%).
The anaemia was later classified as non-regenerative by a complete blood count (CBC). Despite being clinically dehydrated, her urine was isosthenuric, with a specific gravity of 1.011 – ruling out a solely prerenal azotaemia.
The International Renal Interest Society (IRIS) staging system2 (Panel 1) is widely used to identify the severity of renal failure and monitor its progression. A urine protein:creatinine ratio (UPC) of 2.17 showed Bailey had significant proteinuria (>0.5 in azotaemic patients), but, with a blood pressure by Doppler measurement of 150mmHg, hypertension was not a concern.

This information, along with her creatinine level, gave an IRIS staging of 3, substage proteinuric and arterial pressure 1 (low risk of target organ damage). Bailey’s owner had noted the polydipsia and vomiting over several months, suggesting a chronic progression of disease.
The main differential diagnoses for renal failure in such a young patient are summarised in Table 1. Given Bailey’s history and our clinical findings, developmental/juvenile kidney disease was the most likely explanation for her renal failure. An ultrasound scan was used as a non-invasive way to assess renal structure and revealed kidneys of normal size with irregular parenchyma.
The renal pelvis could be visualised, but the cortex and medulla were replaced by tissue of heterogenous appearance, with no distinction between the two areas (Figures 2a and 2b). While a renal biopsy would have given valuable information for diagnosis, this was not carried out due to the risk of worsening renal disease by the biopsy technique itself or the anaesthesia needed to obtain it.


Several studies have been carried out investigating juvenile nephropathies, which have been found to affect more than 20 dog breeds1,3,4,5,6. The condition is believed to be inherited in many breeds, including the shih-tzu, Lhasa apso, Samoyed, cocker spaniel and Tibetan spaniel4,6.
For some, the genetic basis has been identified – in others there have been cases with familial links6. Other factors can also cause renal damage during development or in early postnatal life. These acquired causes include urinary obstruction, vitamin A deficiency, urinary tract infections and some viral infections7.
Often, the result of these genetic or acquired factors is disordered development of the kidney, or renal dysplasia. On histology, this is seen as persistence of fetal kidney components, such as primitive mesenchyme and immature glomeruli and tubules4,5,8. These primary dysplastic lesions will usually be accompanied by secondary changes, such as fibrosis, inflammatory cell infiltrates, cysts and compensatory glomerular hypertrophy4,5,8.
This picture has been seen in more than 20 breeds, including the standard poodle, Lhasa apso, Samoyed and shih-tzu4,6. In some cases, only the secondary changes are seen, which may indicate renal damage without disordered development, or may represent a later stage of dysplasia where fibrosis has obscured the primary dysplastic lesions5,8. It has been suggested inciting causes can rapidly lead to non-specific “end-stage” kidney changes, within as little as 60 days1.
Breeds where dysplastic lesions are less likely to be seen include the miniature schnauzer and Dobermann5,8.
Young boxers seem to have a different pattern of renal disease than other breeds of dog – in fact, the changes have been likened to the human condition juvenile nephronophthisis1,9. Based on the histological lesions and information from human studies, it is suggested renal damage in young boxers is due to reflux of urine from the bladder causing chronic pyelonephritis1,9,10. This may start in utero, causing disrupted development, but continues to progress after birth, even if the reflux and pyelonephritis are corrected. The reflux could be caused by incompetence in the ureteric muscle and a genetic origin has been suggested, but not proven9.

Although we have no histology to confirm it, this reflux nephropathy was most likely the cause of Bailey’s condition.
The point at which clinical signs become evident seems to be very variable – from a few weeks of age up to several years old1,3,4,5,6,8,9. The presenting signs are usually those associated with renal failure – similar to those seen with Bailey, such as polydipsia, polyuria, vomiting, inappetence, isosthenuria and proteinuria1,3,4,5,6,8,9.
The approach to treatment of renal failure is similar in patients of any age, with the aim of stabilising and slowing the progression of renal damage and managing the clinical signs arising as sequelae from renal failure (Table 2).
On initial presentation, Bailey was dehydrated, likely worsening her renal parameters. Intravenous fluid therapy with Hartmann’s solution at 4ml/kg/hour to correct this rapidly improved her demeanour and appetite. She was started on a prescription renal diet to regulate quality and quantity of protein intake, and to restrict dietary phosphate levels. Bailey readily accepted this initially and she was fed a renal diet exclusively for several months. After two days of this initial stabilisation, her urea had fallen to 28.3mmol/L, but her creatinine had risen to 453µmol/L, placing her at IRIS stage 4 (Figures 3 and 4). Despite this worsening of creatinine, Bailey was clinically much improved, with good appetite and normal hydration, so her treatment was continued at home.
As Bailey’s blood pressure remained in an acceptable range – at 150mmHg – we did not need to use antihypertensive medication. If hypertension had developed, amlodipine could have been used for control (off licence). The significant proteinuria did warrant treatment with benazepril at 0.25mg/kg sid per os (PO; off licence in dogs).
After three weeks of treatment at home, Bailey remained bright with a good appetite and had gained 1.5kg in bodyweight. There was some improvement in the azotaemia returning to IRIS stage 3 (urea 16mmol/L, creatinine 400µmol/L) and the proteinuria had improved, with UPC more than halving to 0.95.
Anaemia became a clinical concern when Bailey developed syncopal episodes and the PCV dropped below 25% (Figure 5). It remained non-regenerative and could have several contributing factors. Azotaemia reduces the circulating red blood cell lifespan and also predisposes to gastrointestinal blood loss from gastric ulceration.
In addition, a lack of normal renal tissue leads to reduced erythropoietin (EPO) production and consequently insufficient production of red blood cells even in the face of anaemia. To reduce the risk of gastric ulceration, and because she had developed more persistent vomiting, Bailey was started on the gastroprotectants ranitidine at 2mg/kg bid PO and omeprazole 1mg/kg sid PO (both off licence).
She was also started on a regime to stimulate erythropoiesis with injections of human EPO analogue darbopoietin (off licence). These were obtained by prescription from a medical pharmacy and given SC at 1µg/kg weekly until PCV exceeded 25%, with the eventual aim of reducing frequency and dose to 0.5µg/kg every three weeks long term.

Iron supplementation was given with this regime to support the resulting erythropoiesis. This can be achieved with IM injections, but as these can be painful, we chose to give oral iron sulphate at 200mg sid PO. One notable side effect of this oral iron supplementation is dark, melaenic-appearing faeces.
Bailey responded well to the darbopoietin and, within two weeks, her PCV had risen from 19% to 31% and weakness episodes had reduced. A further CBC showed improvement in haematocrit, but, strangely, did not show much evidence of regeneration. From looking at the literature on some feline cases this is not necessarily unusual11. The possible side effects of darbopoietin use include11:
PCV must be regularly monitored to assess the effectiveness of treatment and highlight any side effects. If darbopoietin was ineffective, or had to be discontinued, the management of anaemia could have been achieved with cross-matched packed cell transfusions every two to three months.
Despite these treatments, Bailey’s azotaemia continued to progress (Figures 3 and 4) over several months and her appetite became more variable. She had some further episodes of acute deterioration requiring intravenous fluids and hospitalisation for a few days.
As the isosthenuria left her susceptible to occult urinary tract infections, urine cultures were performed to check for possible contributing causes to the deterioration. A significant growth of Escherichia coli was found on one occasion and she was treated with potentiated amoxycillin at 12.5mg/kg bid PO based on culture and sensitivity. Other treatments used to maintain her appetite included maropitant at 2mg/kg sid PO, when needed against any nausea, and mirtazepine at 15mg every other day PO, as an appetite stimulant (off licence).
As her appetite became variable and she preferred food in addition to the renal prescription diets, Bailey also had an oral phosphate binder. As there is some suggestion glomerular inflammation can respond to essential fatty acids, we attempted to give her oral omega-3 supplementation, but she did not accept this well and so it was discontinued.
In addition to monitoring the parameters discussed previously (urea, creatinine, PCV, blood pressure, UPC, urine cultures and bodyweight), we also periodically checked albumin and cholesterol. Cases developing hypoalbuminaemia, hypercholesteraemia, oedema and ascites (nephrotic syndrome) have a very poor prognosis.
Throughout Bailey’s treatment, it was very hard to predict how long we could continue to give her a good quality of life. Studies have shown variable disease progression, with survival times varying from months to up to five years from diagnosis1,3,6,9. In some breeds, patterns have been observed – for example, a study of 45 affected shih-tzus showed two main outcome groups, with 22 surviving less than 1 year, but 12 living for more than 4 years after diagnosis4.
In the Samoyed, there is a familial sex-linked transmission through females. As a result, affected males usually have more severe disease and survival times of less than 1 year, whereas affected females can live for more than 5 years6. A review of 37 affected boxers showed a wide range of survival from some euthanised at diagnosis to others surviving more than 5 years1. No clear relationship was found between survival and clinicopathological parameters, such as PCV, UPC or serum creatinine, from the data available1.
In Bailey’s case, she was able to have a good quality of life for six months from her diagnosis. Sadly, at 17 months of age, she deteriorated further and showed no sign of clinical improvement, despite IV fluids. Her owners decided to have her euthanised at this stage.
Renal disease in young animals is becoming more frequently recognised. Although much of the treatment needed is similar to that used for older patients, with renal failure, the prognosis and expectation of the owner are likely to be very different.
The prospect of such young, lively dogs having a shortened lifespan is very difficult for everyone involved, but with committed owners, and a very enthusiastic patient, we managed to give Bailey six months with her family.
Both her owners and myself hope by sharing her case it may give some help for managing other young dogs diagnosed with renal failure.
With thanks to Kevin Murtagh at the University of Liverpool Small Animal Teaching Hospital for invaluable clinical advice on Bailey’s case.