14 Oct 2019
Diego Rodrigo Mocholi details the anaesthetic considerations required for animals with heart disease – from perianaesthesia to recovery.
Diego Rodrigo Mocholi
Job Title
Image: nicole_ciscato / Adobe Stock
Few data are encountered in the literature regarding the prevalence of cardiac disease in small and large animals. Congenital cardiac diseases have shown a prevalence of 0.13% and 0.14% among mixed-breed dogs and cats, respectively.
A study with a population of 111,967 dogs attending 93 veterinary clinics in the UK showed a prevalence of 3.54% of dogs over one year with a recorded heart murmur, which could be consisted with possible or diagnosed degenerative mitral valve disease (Mattin et al, 2015). In equine medicine, mitral regurgitation (4.4%), atrial fibrillation (2.3%), aortic regurgitation (2.1%) and tricuspid regurgitation (1.7%) were the most common cardiac abnormalities detected in a population of 3,434 horses in Liège (Belgium; Leroux et al, 2013).
The cardiovascular system plays as many roles as the diverse tissues and organs it supplies. However, its main function is circulation of blood through the vessels of pulmonary and systemic capillaries for the purpose of exchange of oxygen, carbon dioxide, metabolic nutrients, waste products, and water in the tissues and lungs.
Also, the cardiovascular system has the important role in the distribution of body water between intravascular, extracellular and intracellular spaces; an unbalanced hydrostatic pressure in systemic capillaries facilitates the movement between both the interstitial and intracellular water, and the intravascular space.
The anaesthesia of a cardiac patient could represent a challenge for the clinician, who will need to focus more on describing the specific cardiac disease or cardiac effects of specific anaesthetics and less on their combinations. Then, the practitioner’s knowledge about the pathophysiology of heart disease, good monitoring skills and cardiac medical therapy will help choose the appropriate anaesthetic plan for an individual patient.
A history of the patient and a proper anamnesis will lead the clinician to the differential diagnosis of the cardiovascular disease. Cardiac patients tend to arrive to the consult with a history of coughing, tachypnoea, dyspnoea, cyanosis, hindlimb weakness, exercise intolerance, collapse and/or syncope. Therefore, a comprehensive physical examination is mandatory prior to the anaesthesia of a cardiac patient to guarantee its safety.
Data is also collected from other different cardiovascular diagnoses. Basic auscultation of the thorax and heart is useful to detect abnormal sounds (for example, murmurs or crackles). Arrhythmias are normally recorded by direct pulse palpation and ECG. Echocardiography is useful to assess the dimensions of the different heart chambers and important vessels.
Thoracic radiographs can be performed in conscious stable cardiac patients with a history of tachypnoea or dyspnoea, suspicious of pulmonary oedema, left-to-right shunting cardiovascular anomaly or when pulmonary thromboembolism is suspected.
After data collection, cardiac patients undergoing an anaesthetic procedure are classified following the next points:
Any stress must be avoided in the cardiac patient. Patients with a cardiac disease are more sensitive to the release of catecholamines after any excitement situation due to its minimal ability to compensate for cardiovascular alterations.
Preoxygenation before anesthetic induction and tracheal intubation is a widely accepted manoeuvre. The use of a high fraction of inspired oxygen with either direct flow or a tight mask (if it is well tolerated by the patient) during three to five minutes is designed to increase the body oxygen stores, and thereby delay the onset of arterial haemoglobin desaturation during apnoea. Because of difficulties to compensate during cardiovascular instability and to reduce myocardial hypoxia, the need for preoxygenation is desirable in cardiac patients.
Cardiac patients are normally stabilised at home with oral medication to decrease severity of the cardiovascular disease. Nowadays, some controversy exists about the interruption of this medication, which could cause few side effects that may be exacerbated during the anaesthesia maintenance. It is recommended in veterinary medicine to discontinue the treatment with angiotensin-converting enzyme inhibitors, which are responsible to induce refractory hypotension.
Calcium channel inhibitors and beta blockers are often interrupted on the day of anaesthesia due to its negative effect on contractility and heart rate. The decision to withdraw diuretics is based on practitioner opinion and individualised in each case according to the specific risk of developing oedema.
Severe cardiac disease patients either may not be stabilised at home or are referred to the hospital as an emergency situation, and then initial aggressive therapeutic and supportive plan are necessary. Furosemide (2mgkg-1 IV up to every one to two hours; maximum total dose of 8mgkg-1) is normally administered to reduce and control of pulmonary oedema. Pimobendan IV administered in dogs (0.15mgkg-1 to 0.3mgkg-1) reduces both afterload and preload, while improving myocardial contractility.
It is recommended to drain completely pleural and pericardial effusions. However, complete drainage of ascites is controversial because it can result in electrolyte imbalances and hypoproteinaemia. Nevertheless, if the amount of ascites is massive and severe then partial drainage may help reduce intrabdominal pressure, which decreases the pressure effect on the diaphragm and improves ventilation.
Acepromazine is one of the most widely used phenotiazines in veterinary practice. The sedative effects are mediated primarily by blockade of dopamine receptors. Also, the blockade of alpha 1 adrenergic, muscarinic and histamine receptors play a role in sedation. The disadvantage after administration of acepromazine is the dose-dependent reduction in stroke volume, cardiac output and arterial blood pressure.
The effect on arterial blood pressure is due to a peripheral vasodilation mediated by alpha 1 adrenergic receptor antagonism. However, acepromazine has the beneficial property to desensitise the myocardium against the arrhythmogenic effects of catecholamines, which is helpful to reduce the likelihood of ventricular arrhythmias.
Alpha 2 adrenergic agonist receptors (xylazine, detomidine, romifidine, medetomidine and dexmedetomidine) provide sedation, analgesia and muscle relaxation. One important advantage is its reversal with administration of selective antagonists (atipamezole). These drugs cause a severe effect on the cardiovascular system. Initially, alpha 2 adrenergic agonists receptors cause an intense peripheral vasoconstriction, which leads to a mediated baroreceptor (vagal) reflex and bradycardia.
This severe increase in the systemic vascular resistance decreases the sympathetic outflow from the CNS, and it enhances the persistence of bradycardia. Besides, the reduction in heart rate as a reflex to maintain physiological blood pressure after the increased systemic vascular resistance causes a reduction in the cardiac output.
Benzodiazepines (diazepam and midazolam) exert their sedative effects in the CNS by enhancing the gamma-aminobutyric acid (GABA) A receptor’s affinity for GABA, resulting in increased chloride conductance and hyperpolarisation of postsynaptic cell membranes. Benzodiazepines are a preferable choice for cardiac disease patients because they have minimal to no effects on hear rate, contractility or vasomotor tone, and, therefore, an induced hypotension is avoided.
However, benzodiazepines are considered to have very light sedative potency, and may even produce paradoxical excitation if they are not associated with other drugs with greater sedative power. Nevertheless, severe cardiac disease patients may be depressed; therefore, the induced overexcitation by benzodiazepines is minimal.
Opioids given at clinical doses have minor direct effects on the cardiovascular system in veterinary medicine. An increase of the parasympathetic activity (vagal tone) in neurons innervating the heart causes a dose-dependent decrease in heart rate. During mild bradycardia, an increase in stroke volume maintains normal values for cardiac output. However, if severe bradycardia occurs, the administration of anticholinergic drugs is recommended to reverse this effect. Minor increases or decreases in systemic vascular resistance and arterial blood pressure have been shown after opioid administration. The more profound effect on vascular system is normally associated with the IV injection of high doses of morphine, which is thought to be mediated by histamine release from mast cells.
For cardiac disease patients undergoing general anaesthesia, the use of locoregional anaesthesia and analgesia techniques are of great value to reduce injectable and inhaled anaesthetic drug doses. Local anaesthetics block the generation and propagation of electrical impulses in peripheral nerves by acting primarily on sodium channels.
Although an antiarrhythmic effect occurs at low concentrations, most local anaesthetics may produce cardiac toxicity at higher concentrations.
Thiopental leads to few side effects after causing a generalised vasodilatory effect in the body system. Although a mild hypotension state is induced by vasodilation, a reflex increase in heart rate tends to compensate. A decrease in PCV and enlargement of the spleen can be seen due to sequestration of red blood cells in the spleen after venodilation. Vasodilation of cutaneous and skeletal blood vessels predispose the patient to hypothermia. Also, a reduction in stroke volume and myocardial contractility have been seen after administration of lower doses of thiopental. Medium to high incidence of arrhythmias can be recorded in the patient as thiopental sensitises the myocardium.
Dose-dependent decreases in arterial blood pressure, systemic vascular resistance and cardiac output are common side effects after propofol administration. These cardiovascular effects may be more profound in patients that are hypovolaemic, geriatric or have compromised left ventricular function.
Stimulation of the sympathetic nervous system outflow leads to an increase of systemic and pulmonary arterial pressure, heart rate, cardiac output, myocardial oxygen requirements and cardiac work re-seen after IV administration of ketamine. Ketamine increases concentration of plasma catecholamines by inhibition of norepinephrine reuptake. However, ketamine should be used with caution in patients with severe cardiovascular disease and those that are already tachycardic and/or dysrhythmic.
Alfaxalone administered at clinical doses does not cause any detrimental effect in the cardiovascular system in animals. However, higher doses of IV administration of alfaxalone produces a direct negative effect in heart rate, arterial blood pressure, and cardiac output in dogs and cats.
Stability in heart rate, stroke volume, cardiac output, mean arterial blood pressure, central venous pressure or cardiac index have been seen after etomidate administration.
A direct myocardial depression and a decrease in sympathoadrenal activity effect from all volatile inhalation anaesthetics are the reason for the dose-dependent effects in the cardiovascular system. Newer volatile anaesthetics tend to preserve cardiac output at clinically useful concentrations, facilitated by reductions in systemic vascular resistance. However, a dose-related decrease in blood pressure exists related to a decrease in stroke volume and, in some cases, a decrease in peripheral vascular resistance.
IV administration of anticholinergic drugs is used as therapy of bradycardia, and typically leads to an increase in sinus rate, acceleration of atrioventricular nodal conduction and increased atrial contractility.
Increases in myocardial contractility, heart rate, cardiac output and coronary blood flow are the predominant effects of dopamine administered at lower rates. At greater rates, an increased systemic and pulmonary vascular resistance, venous return and PCV exists. An increase in cardiac output due to an improvement in cardiac contractility is the main effect after dobutamine administration. Also, dobutamine has a positive inotropic and chronotropic effect. Ephedrine increases cardiac output, heart rate, blood pressure, coronary blood flow and myocardial oxygen consumption. However, these effects may be transient, and a repeat dose can be ineffective due to its tachyphylaxis.
Norepinephrine increases heart rate and cardiac output, and decreases in systemic vascular resistance at lower doses. A dose-dependent increase in systolic, diastolic and mean arterial blood pressures, cardiac output and systemic and pulmonary vascular resistance have been seen at higher doses.
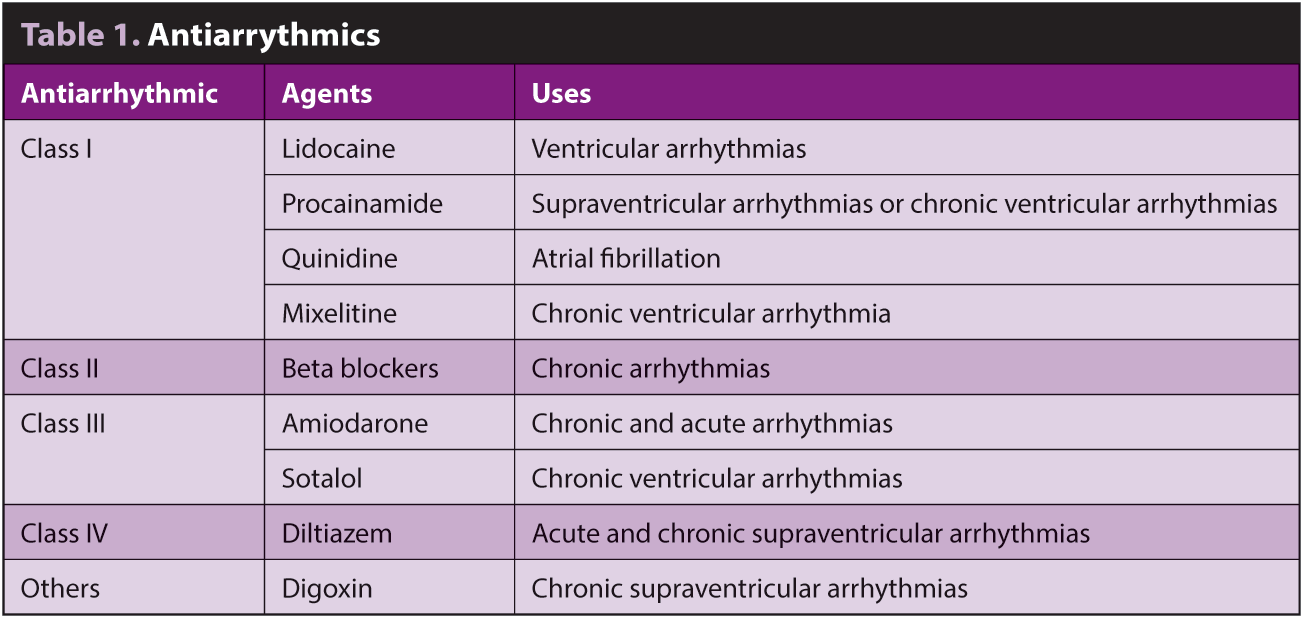
Also, norepinephrine increases coronary blood flow due to a coronary vasodilation. An increase in systemic vascular resistance and mean arterial blood pressure are the common effects after phenylephrine administration. Positive inotropic without increasing myocardial oxygen demand, lusitropy and vasodilatory effects after pimobendane administration. Anti-arrhythmics are described in Table 1.
During the recovery phase, the clinician should not forget the continuous monitoring of the patient with a cardiac disease. The following points describe some of the guidelines to follow during this final phase of the anaesthesia: