23 Oct 2017
Francesco Cian describes the case of a rapidly growing mass in the anal sac of an adult male English cocker spaniel in his latest Cytology Corner column.
Francesco Cian
Job Title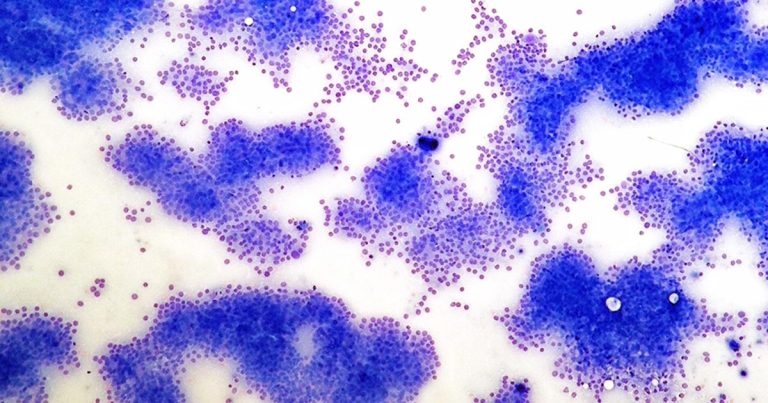
These images are from a rapidly growing mass in the anal sac of an adult male English cocker spaniel (Wright-Giemsa, 10× to 50×). What is your diagnosis?
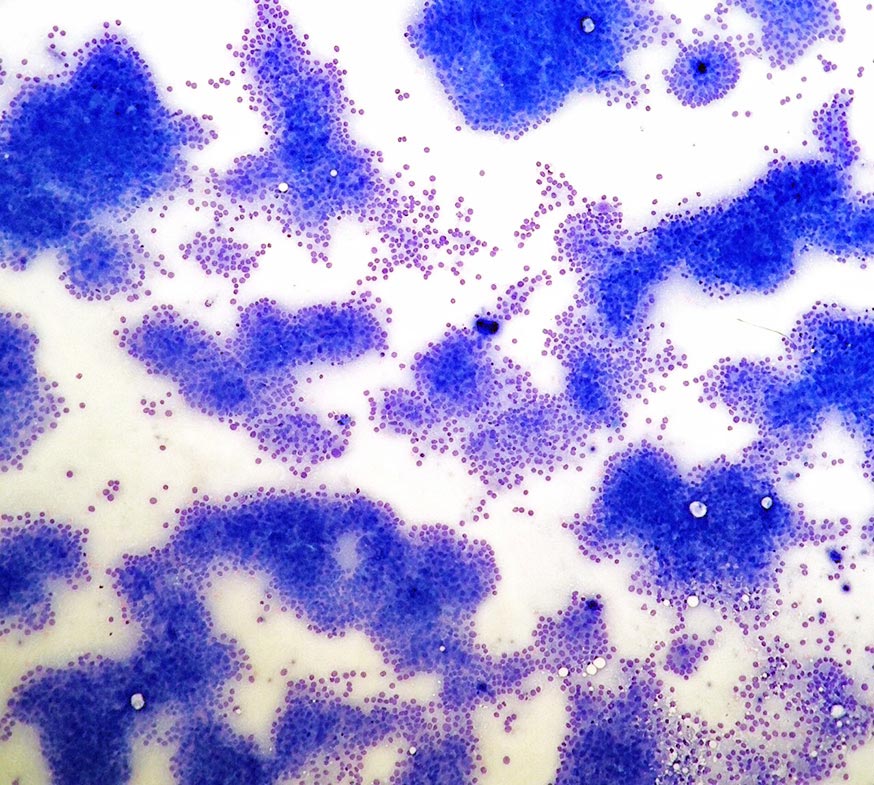
The submitted sample is highly cellular, with moderate preservation. A lightly basophilic background with small numbers of red blood cells is present.
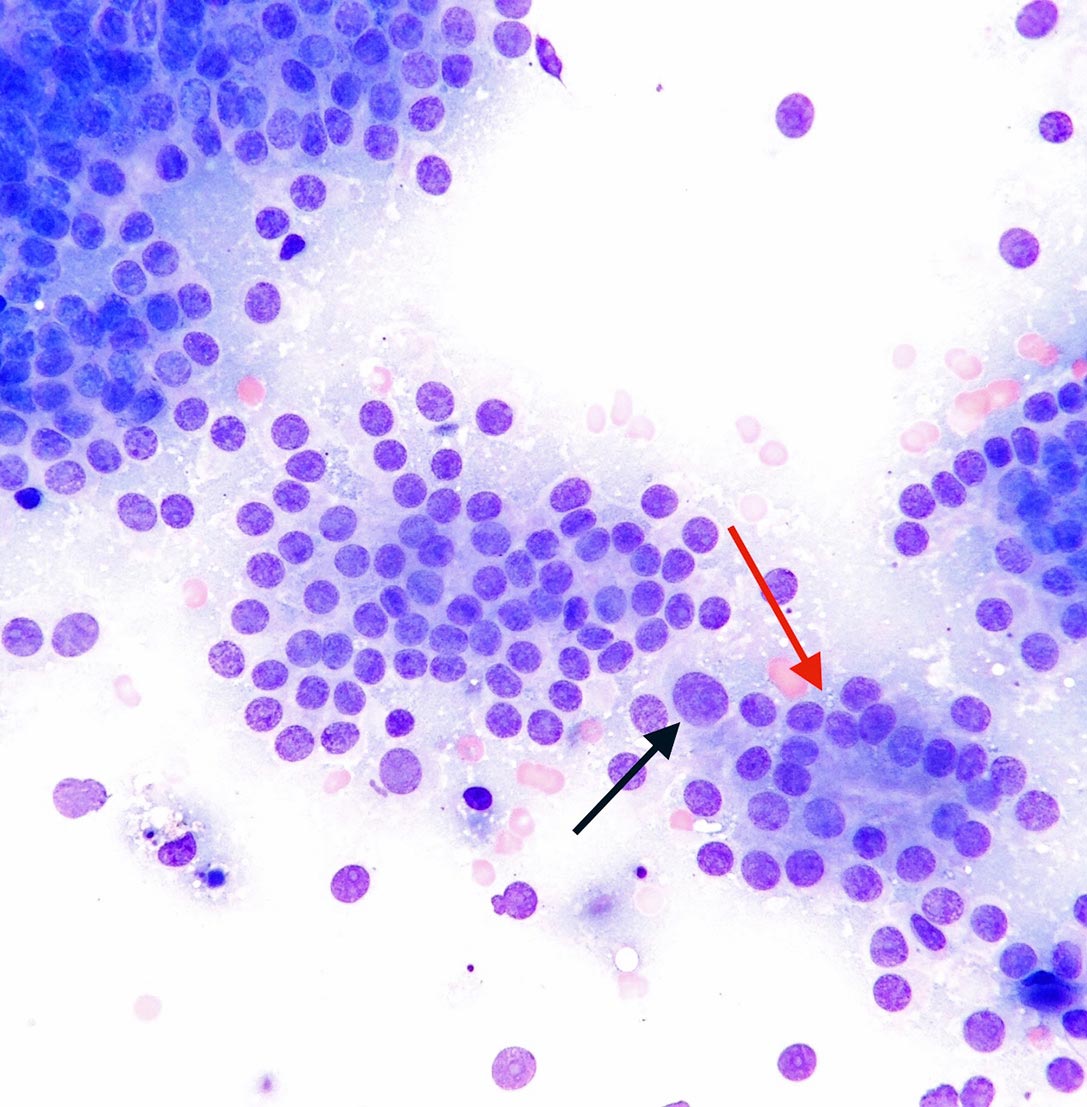
High numbers of nucleated cells are seen throughout the smears and appear as bare nuclei embedded in a background of lightly basophilic cytoplasm, with infrequent appearance of cytoplasmic membranes. They often form clusters of variable sizes and rarely show an acinar arrangement (red arrow).
Nuclei are round, with granular chromatin and indistinct nucleoli. Anisocytosis (cell size variation) and anisokaryosis (nuclear size variation) are mild; occasionally moderate (black arrow). Rare blood-derived neutrophils and scattered foamy macrophagesare also noted.
These findings are consistent with anal sac adenocarcinoma.
The submitted aspirate harvested a main population of epithelial cells arranged in clusters (and acini), which is consistent with a lesion of epithelial (glandular) origin. The cytological featuresof these cells, together withthe location of the mass, are, overall, supportive of an analsac adenocarcinoma.
Despite the mild/moderate cytological features of atypia, this tumour is considered to be clinically aggressive. Anal sac adenocarcinomas are neoplasms arising from the apocrine secretory epithelium found in the wall of the anal sac; the benign counterpart (adenoma) is rare.
These neoplasms are commonly observed in adult/old dogs, with English cocker spaniels being overrepresented. They appear as intradermal/SC, exophytic masses – often ulcerated – in the ventrolateral aspect of the anus. Large masses may impinge on the rectum, resulting in straining and difficulty in defecation.
However, these tumours are often occult or very small, and only found on rectal palpation; therefore, at the time of diagnosis, a large percentage of cases will show metastatic spread in the pelvic canal and/or to the sacral and iliac lymph nodes. Other sites of metastases include the lungs, liver and spleen.
Paraneoplastic hypercalcaemia is reported in a variable percentage of cases (25% to 50%), and may result in polyuria, polydipsia and weakness. It is secondary to the tumour secretion of parathyroid hormone-related peptide.