6 Jan 2025
Hannah van Velzen reviews the most up-to-date knowledge available on this challenging disease in dogs.
Hannah van Velzen
Job Title
Image: © Valeriia/ Adobe Stock
Commonly referred to by its abbreviation, and previously known as canine ulcerative paradental stomatitis, canine chronic ulcerative stomatitis (CCUS) can be a frustrating and challenging disease to manage.
Even milder presentations of this oral inflammatory disease can result in severe levels of pain, and with the exact cause still being unclear, management options are limited and liable to change as new research comes to light. In this article, we will review the current and most up-to-date knowledge available on this debilitating disease, including new recommendations for treatment.
Previously, CCUS was commonly characterised by the presence of “kissing lesions”. These are areas of mucosal inflammation and ulceration located in areas where these tissues lie in direct contact with plaque on tooth surfaces. Though this may be a classic presentation, it has been shown to not be pathognomonic, and lesions may also be found on pretty much all other surfaces in the oral cavity. This includes (but is not limited to) the lateral and ventral tongue surfaces, the gingiva, the hard and soft palate, and any mucocutaneous junctions1.
Approximately 40% of lesions occur in edentulous areas2, which is what has prompted a move away from the term “paradental stomatitis”.
Lesions can vary significantly in their severity, meaning they may present as erosions, white striae, ulcers, pseudomembranous inflammation and/or areas of necrosis. Due to the wide variation in appearance, differential diagnoses should, as a minimum, include chemical burns, lupus erythematosus, pemphigus vulgaris, bullous pemphigoid, erythema multiforme, epitheliotropic lymphoma and uraemic stomatitis.
An increased prevalence of CCUS has been reported in the Maltese, cavalier King Charles spaniel, Labrador retriever, greyhound and terrier breeds1. In the author’s experience, cocker and springer spaniels also seem to be common patients, though this is yet to be supported in literature.
Dogs with CCUS are typically quite painful, may struggle or refuse to eat, and can exhibit significant behavioural changes associated with chronic pain. Owners are also likely to report halitosis, salivation and weight loss.



Considering the amount of differentials, a thorough work-up is essential to allow for proper diagnosis and further treatment of patients with suspected CCUS. Besides a general clinical examination, a standard blood panel is usually recommended as part of the initial work-up. Although complete blood counts and biochemistry are generally unremarkable in these patients, it is important to rule out any significant systemic disease that may present with oral ulceration – particularly end-stage renal disease.
Conscious oral examination may be very difficult due to the level of oral pain these patients experience; therefore, a detailed assessment will almost always require a general anaesthetic with provision of appropriate analgesic premedication and even local anaesthesia if required.
It is recommended patients are assigned a canine ulcerative stomatitis disease activity index (CUSDAI) score1 at the start of the first procedure, prior to any interventions being undertaken.
This scoring system was described by Anderson et al in 2017 and is based on a similar scoring used for feline chronic gingivostomatitis. It is a combination of a subjective owner scoring and an objective scoring of ulcer number, size, location and characteristics. Performing this scoring helps to quantify the severity of disease and, moreover, is an important tool for objective monitoring of response to treatment at the time of repeat examination.
After CUSDAI scoring has been performed, a detailed oral examination, including probing of all teeth and full mouth dental radiography, is the next step. Although CCUS has not been linked to any specific or pathognomonic radiographic findings1, this detailed oral examination should detect oral comorbidities such as periodontitis, which are likely to influence treatment recommendations for the patient as a whole. Localised grade 2 periodontitis is a common finding in dogs with CCUS1.
The only way to definitely diagnose CCUS at present is through a combination of clinical examination and histopathology. Biopsies of affected oral mucosa can be collected easily with use of biopsy punches (minimum 5mm diameter recommended, ideally 8mm to 12mm) and should include perilesional “normal” tissue to help differentiate the presentation from various autoimmune disorders. Ideally, submucosal and connective tissue would be included in the sample.
If possible, photographs, radiographs and a complete clinical history should also be supplied to the pathologist. Oral histopathology can be notoriously challenging to interpret; therefore, it is recommended to use a laboratory with pathologists that have a special interest in and experience with oral histology3.



A specific trigger for, or underlying cause of, CCUS is yet to be identified, but the research performed so far has given us some clues at least. Historically, it was hypothesised that CCUS was an aberrant immune response to plaque present on the tooth surfaces. Current literature, however, does not seem to support this theory.
Although consistent across cases of CCUS, leukocyte numbers and distribution within mucosal lesions differ from that of healthy tissues and from those with advanced periodontitis lesions2.
Further evidence against a plaque-mediated pathogenesis was provided through next-generation sequencing analysis of the biofilm present on CCUS lesions. This was shown to be significantly different from not only that of the opposing tooth surfaces, but also from normal oral tissues and advanced periodontitis lesions4. These results suggest an immune-mediated inflammatory disease rather than a plaque-responsive disease2.
CCUS lesions are characterised by dense, lichenoid, plasmacytic-lymphocytic infiltrates at the interface between mucosal epithelium and subepithelial connective tissue, the transition between these layers often being obscured by the degree of inflammation.
Common findings include epithelial degeneration with more pronounced changes in areas of more severe inflammation, basal cell vacuolisation and apoptosis, epithelial cell degeneration/spongiosis, granulomatous changes, perivascular inflammation, suppurative inflammation, necrosis in the subepithelium and pseudomembrane formation. Abundant subepithelial mast cells are also identified in most lesions. Individual keratinocyte necrosis in the stratum spinosum, pigment incontinence and dyskeratosis are less commonly reported1.
Depending on the exact presentation, CCUS appears as one of three histological subtypes: lichenoid stomatitis, deep stomatitis and granulomatous stomatitis. Whether this represents a continuum of the same disease process or distinct variants of the disease is yet to be determined1.
In an attempt to further define the pathogenesis, immunofluorescence has helped rule out an autoantibody-mediated autoimmune disease and confirmed the presence of specific cell subtypes, cytokines and messenger proteins that may indicate dysregulation of the immune system. CD79a+ B-cells, CD3+ T-cells and regulatory T-cells are the most common, alongside FoxP3+ and IL17+ cells.
Interestingly, in contrast to other inflammatory cells identified in CCUS lesions, IL17+ cells are inversely correlated to the CUSDAI score, suggesting a possible protective roll2.
These subsets and subtypes of cells present in CCUS lesions have been shown to differ from that of feline chronic gingivostomatitis, which was long considered to be a very similar disease in another species.
Historically, partial and full-mouth extractions have been recommended for treatment of CCUS.
However, as described previously, the evidence is not supportive of a plaque-responsive disease process, which explains why this treatment does not have a 100% success rate. The newest recommendations, therefore, include only extraction of “hopeless” teeth (such as those with end-stage periodontal or endodontic disease). Professional dental cleaning and periodontal therapy of teeth with mild periodontal disease is still strongly recommended to reduce overall and general oral inflammation levels.
General oral microbe level reduction may disrupt or prevent formation of the unique microbiome found on CCUS lesions, and ongoing home care is still a cornerstone of management. However, oral pain may prohibit owners from providing any level of oral care postoperatively.
Medical treatment should, therefore, always include sufficient amounts of multimodal analgesia. Where disease and oral pain is severe, oesophageal feeding tube placement may need to be considered to allow for nutritional support and consistent administration of medication until improvement can be achieved.
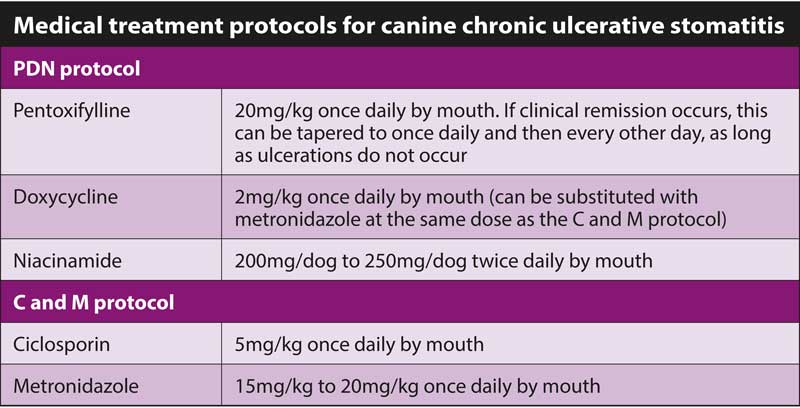
Based on our level of knowledge of the presentation of and cellular types involved in CCUS, two specific drug combination options have been proposed and are increasingly being used for medical management.
A short description of the rationale behind both protocols is given in the following section. Which protocol to initiate is often a matter of clinician preference.
Most dogs will require lifelong treatment, whereas others may be able to taper medications if, and once, resolution of signs has occurred.


Pentoxifylline reduces inflammation through numerous mechanisms, including inhibition of inflammatory cytokine production, reduction of lymphocyte proliferation and neutrophil adhesion, increasing of erythrocyte flexibility and blood vessel dilation, and antioxidant activity.
Tetracycline antibiotics, including doxycycline when used at a sub-antimicrobial dose of 2mg/kg, have the ability to inhibit matrix metalloproteinases and, therefore, serve an important role in modulation of the inflammatory response.
Niacinamide, also known as vitamin B3, has various functions in maintaining the balance between physiologic and pathologic inflammation of the oral cavity.
Ciclosporin is an immunosuppressive agent that inhibits T-cell function and suppresses cell-mediated immune responses by reducing the production of various cytokines.
Similar to doxycycline, metronidazole is used for its immunomodulatory functions. It slows the proliferation of lymphocytes, reduces leukocyte migration from the bloodstream, and inhibits antibody production by B-cells.
Components of the CCUS microbiome may also be more susceptible to metronidazole. In addition, both medications interact with the P-450 enzyme system, suggesting the potential for a synergistic relationship.
In a small pilot study, this protocol was shown to be quite effective in improving CUSDAI scores within only three weeks. Over the study period of six months, the majority of owners in a group of 10 dogs reported an overall 90% to 100% improvement.
However, 50 per cent of dogs experienced side effects from the medication, most commonly minor and manageable gastrointestinal symptoms5.


While many questions remain, and research is only just starting to provide insights into this complex disease, recent findings have resulted in a significant shift from recommending a primarily surgical approach in the CCUS patient to recommending a more tailored evaluation and medical management.
It is likely that as further literature is published and other treatment protocols are explored, these recommendations will continue to evolve, hopefully allowing us to provide these complex and painful patients with a significantly better quality of life.