2 Nov 2015

Figure 1. The more clinical signs a dog has of hyperadrenocorticism the lower the thresholds required in endocrine testing for the diagnosis of this condition. In particular, the presence or absence of polyuria (as shown) is important, but other conditions that can cause this clinical sign need to be excluded.
Making a confident diagnosis of canine hyperadrenocorticism (HAC) can be a challenge. This may be because patients are now being investigated earlier in the course of disease and signs may not be as pronounced as when the disease was first described.

Many dogs also have concurrent conditions or are receiving medication that can complicate the diagnosis.
Knowledge of the distinct types of HAC is helpful for deciding on the most efficient diagnostic approach. The most common HAC (between 80 to 85% of cases) is pituitary-dependent hyperadrenocorticism (PDH), which is the result of over-secretion of adrenocorticotropic hormone (ACTH) from the pituitary gland. Most cases of PDH are caused by a microadenoma, but around 10% to 15% of cases have a macroadenoma. Alternatively, HAC can be adrenal dependent (ADH), usually caused by a unilateral adenoma or carcinoma (occurring in equal frequencies).
The signalment, clinical signs and results of clinicopathological testing (including haematology, biochemistry and urinalysis) are discussed in detail in several textbooks (see reading list). Common and uncommon clinical signs are shown in Table 1 and expected clinicopathological alterations are shown in Table 2. Middle aged to older dogs of breed, size and either sex can be affected, but females may have a slightly increased risk.
The importance of taking a complete history, performing a thorough physical examination, haematology, biochemistry and urinalysis cannot be over-emphasised. Many conditions can mimic some or all the signs of HAC (for example, diabetes mellitus, hypothyroidism and renal failure) and it is essential to exclude them, before continuing with specific testing (Figure 1). In contrast, the lack of expected abnormalities on physical examination or basic clinical pathology testing, while not excluding HAC as a possibility, significantly reduces the likelihood of the disease.

Diagnostic imaging should always be performed before starting any treatment for HAC and usually before specific endocrine testing. Radiographs of the abdomen can be helpful, with identification of hepatomegaly likely and, in some cases, radiopaque uroliths (Figure 2). Calcified adrenal masses can be present; however, they are only seen in 50% of ADH cases.
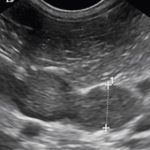
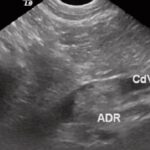
Adrenal ultrasound is more informative, but identification of these glands requires practice. Dogs with suspected/confirmed HAC can offer a good chance at improving this skill. In PDH, the adrenal glands are typically symmetrically enlarged and normal in shape, size and echogenicity (Figure 3). In ADH, normally a unilateral adrenal mass is detected, which is unusual in shape and echogenicity (Figure 4), with the contralateral adrenal gland typically small. Adrenal gland masses can also be invading or compressing adjacent structures, such as the caudal vena cava (Figure 5). General abdominal ultrasonography is also useful, but beware over-interpreting the many age-related changes and those secondary to the underlying condition, such as splenic nodules and a patchy hyperechoic liver.
Endocrine testing should be the final diagnostic step, not the first. If the clinician is armed with the information from routine blood screens and diagnostic imaging before performing endocrine testing then interpretation of the results and confirmation or exclusion of the disease is easier.

Several tests are available, which can confuse and frustrate in equal measure. When selecting a test or tests to perform, it is important to consider their varying sensitivities and specificities, which are in turn influenced by the likelihood of HAC in that particular population, concurrent medication, acute stress and disease.
Concurrent drugs such as glucocorticoids, metoclopramide, desmopressin and buprenorphine can affect the hypothalamic-pituitary-adrenal axis. Therefore, if a patient is receiving such medication, it is prudent to withdraw (when possible) before commencing endocrine testing. In the case of glucocorticoids, the time needed between withdrawal and testing varies depending on the dose, frequency and duration.

Various techniques are available to measure cortisol, including radioimmunoassay, ELISA and chemiluminescence. The assay type has a significant impact on cortisol results. Results can even be inconsistent between laboratories using the same method, with the magnitude of discrepancy being, in some cases, clinically significant. Many laboratories now take part in quality control schemes such as that run by the European Society of Veterinary Endocrinology. Veterinary surgeons should ensure the laboratory they send samples to are involved in such schemes before trusting the results. In-house assays require similar levels of quality control (which are, sadly, rarely done) to achieve the same level of confidence in their results. Reference ranges are individual to each laboratory and are not interchangeable.
The low dose dexamethasone suppression test (LDDST) is the test of choice for diagnosing HAC, especially in the current climate of reduced tetracosactide availability. It is very sensitive (90% to 95%) and moderately specific (44% to 73%) depending on the population of dogs tested. False positives can occur in patients with non-adrenal illness and this test should be reserved for those cases with a reasonable index of suspicion, after other non-adrenal illnesses (such as diabetes mellitus and renal failure) have been excluded.

If a patient is suspected to have HAC and is concurrently unwell (for example, with another related or unrelated condition), testing should be delayed until recovery. Even acute mild stress (such as an ultrasound) could affect the results, depending on the timing relative to blood sampling. The authors therefore recommend no other investigations are performed on the day of the test. The patient’s demeanour and response to environmental stimuli should also be taken into account.
The diagnosis is based on the cortisol result obtained eight hours after administration of dexamethasone, and the cut-off value varies between laboratories and depends, to some extent, on the severity of the clinical signs and other clinicopathological tests. Seeking advice from more experienced colleagues is an inexpensive way of increasing the diagnostic yield of endocrine tests.
Occasionally, an “inverse” pattern is seen, when the result obtained at three or four hours after administration is above the cut-off for diagnosis, but the result at eight hours is below. This pattern is suspicious for HAC, but further testing (that is, repeating the LDDST or pursuing alternative tests) is recommended.
The ACTH stimulation test, measuring cortisol before and after 5µg/kg of tetracosactide is administered, is the least sensitive (between 60% to 85%) and most specific (59% to 93%) test for HAC. False positives are not as frequently encountered as with the LDDST, tending to occur with more severe non-adrenal illness (such as diabetic ketoacidosis).
Acute stress is less likely to affect the results. In ADH, the sensitivity is lower when compared to PDH; however, when the test is performed clinically, this distinction may not yet have been made. If a dog has a positive or, in some circumstances, a borderline result, with compatible clinical signs and results of previous investigations (including exclusion of other conditions), it is extremely likely to have the HAC.
The UCCR is the most sensitive test (75% to 100%); however, it lacks specificity (20% to 25%). Assays available in the UK are considerably different from those available in some European centres. This is because of variation in antibody configuration, which results in a decrease in the specificity of the test within the UK.
Although the UCCR will be positive in the majority of dogs with HAC, dogs with other unrelated non-adrenal
illnesses and experiencing acute stress (such as examination or hospitalisation) can also test positive.
To reduce the risk of a misdiagnosis, it is best to perform the test on two or even three morning samples collected at home and pooled in equal volumes. Given the problems encountered with the test, the UCCR is used by the authors primarily to exclude HAC.

It is important to consider differentiation between ADH and PDH as this has implications for the treatment, prognosis and possible eventual sequelae of the condition. For example, adrenal tumours can be treated by adrenalectomy, whereas in some cases of PDH, radiotherapy may be an option if caused by a pituitary macroadenoma. If ADH is treated medically with trilostane then it has a poorer prognosis compared to dogs with PDH.
The results of the three or four hours post dexamethasone cortisol result obtained during a LDDST can be helpful. If suppression occurs (either less than 50% of baseline cortisol and below the laboratory cut-off – often 40nmol/L) then a diagnosis of PDH can be made. This only occurs in 65% of cases of PDH and a lack of suppression at three or four hours means this distinction cannot be made. The high dose dexamethasone suppression test is now considered an out-moded, imprecise, time-consuming and expensive test compared to the alternatives such as endogenous ACTH.
The measurement of endogenous ACTH (eACTH) is based on the principle dogs with ADH normally have low/undetectable levels, whereas in PDH levels are normal or high. Up to 20% of dogs can have eACTH levels too low to be considered compatible with PDH, but too high to be consistent with ADH, which can be frustrating, but it remains the most accurate standalone test. Specific sample handling is required, including freezing of an ethylenediaminetetraacetic acid sample within 15 minutes and frozen shipment. External laboratories can often assist with this, providing guidance and practical support.
Imaging can be helpful – for example, calcification of the adrenals on radiographs and appearance of adrenals on ultrasound. Imaging of the pituitary gland by MRI or CT could be considered, even in cases where neurological signs are absent, especially if considering radiotherapy or hypophysectomy. This is because macroadenomas (Figure 6) can be present without neurological signs, and both radiotherapy and hypophysectomy are more effective in cases with smaller tumours and absent neurological signs.
Before reaching a diagnosis of HAC, it is essential to exclude other conditions. Most dogs with the condition are well, but occasionally patients can be unwell, directly attributable to the disease.
The most common example is probably pancreatitis, which is a frequent initial presentation of HAC in the author’s clinic. Other examples include pituitary macroadenoma, causing reduced appetite or mentation, which can happen at the initial presentation or many months after treatment.
Dogs can also become hypercoaguable, with some developing life-threatening complications such as a thromboembolism. Due to the acute metabolic stress this group of patients may be experiencing, interpretation of endocrine test results is fraught with difficulty. These scenarios are not common and investigation (and indeed, treatment) for HAC, even if it is suspected to be the underlying aetiology, should be withheld until stability has been achieved.
Thorough case evaluation and a logical work-up should ensure the diagnosis of HAC is achieved without stress. The treatment of HAC, whether medical or surgical, can be costly and a complete investigation before starting this treatment does not add significantly to this when compared to the costs of misdiagnosis. Should this investigation identify another condition as well as HAC, then the long-term costs and risks associated with treatment are also reduced.
Differentiation of the type of HAC present is an important final step once the diagnosis is reached, before embarking on treatment.