12 Jun 2017
Francesco Cian presents on the case of an eight-year-old female dog with generalised lymphadenomegaly.
Francesco Cian
Job Title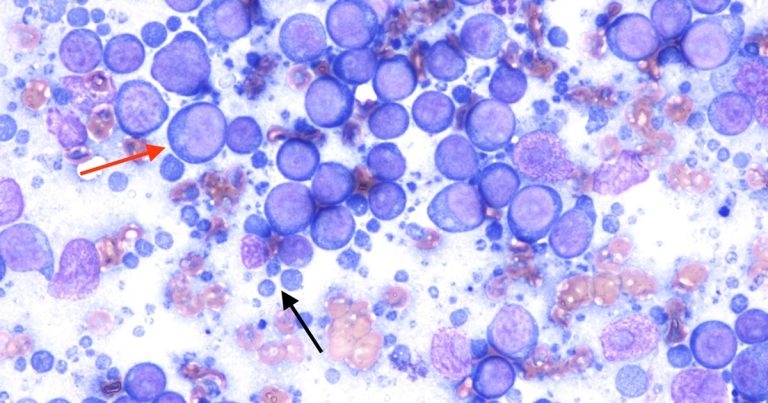
Cytology pictures from an aspirate of an enlarged prescapular lymph node in an eight-year-old, female dog.
The pictures to the right are from an aspirate of an enlarged prescapular lymph node in an eight-year-old, female dog with generalised lymphadenomegaly (Wright-Giemsa, 100×). What is your diagnosis?
The submitted sample is highly cellular, with adequate preservation. The background is clear, with low numbers of red blood cells and high numbers of rounded, light-to-dark blue cytoplasmic fragments, also named as lymphoglandular bodies (black arrow).
A main population of mainly large lymphoid cells is present (red arrow), which have moderate amounts of deep blue cytoplasm, with defined borders, and a large, paracentral nucleus (more than 2.5 red blood cells), with coarse granular chromatin, and up to three, prominent, round nucleoli.
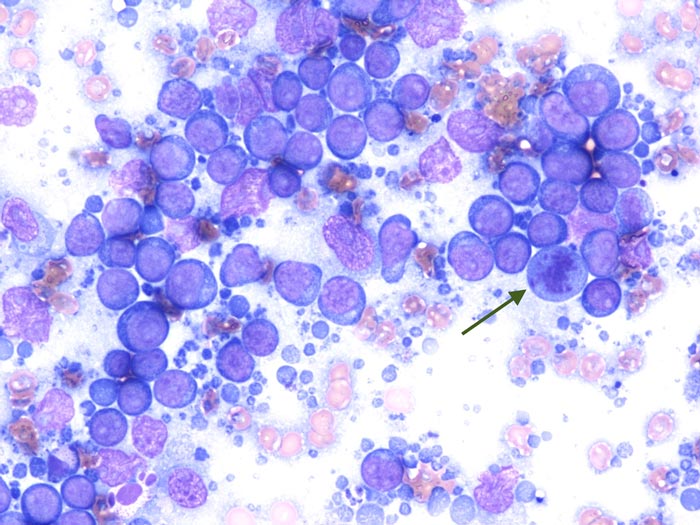
Occasional atypical mitotic figures are present (green arrow), and rare small lymphocytes and a few blood-derived neutrophils are also noted.
In the submitted aspirate, you can appreciate the presence of a monomorphic population of large lymphoid cells, which accounts for more than 80% of all cells.
Together with the clinical history of a generalised lymphadenomegaly, these findings are supportive of lymphoma – and, more specifically, a high-grade large cell form.
No additional investigations are needed in this case to confirm the diagnosis of lymphoma, but further testing may be helpful to further characterise the process.
T-cell phenotype, for example, has been reported to be a negative prognostic factor in high-grade multicentric canine lymphomas,and is associated with shorter remission and survival durations (Valli et al, 2013).
Immunophenotyping can be achieved with several diagnostic techniques, including flow cytometry and immunohistochemistry – the latter requiring a solid biopsy.
Flow cytometry was performedon a new, fresh lymph node aspirate and the above population was positive to CD79a and CD21, bothof which are B-cell markers, confirming the diagnosis of a diffuse large B-cell lymphoma, according to the World Health Organization classification for neoplastic diseases of the lymphoid tissues.
Diffuse large B-cell lymphoma is the most common subtype of canine lymphoma, accounting for almost 50% of lymphomas in this species. It often has a multicentric presentation with a generalised lymphadenopathy. In advanced cases, other internal organs (for example, the spleen or liver) canbe involved.
When circulating neoplastic cells are seen in the peripheral blood and the bone marrow is effaced by the neoplastic population, the lymphoma is defined as stage V or leukaemic.