30 Nov 2015
Shasta Lynch
Job TitleWhen a patient is diagnosed with cancer, the first step is to seek advice from a veterinary oncologist. This establishes a plan for the patient, comforts the owner and allows you to discuss ongoing diagnostics and treatment with him or her at length.
If you choose to refer the patient at this point, you may offer to administer chemotherapy treatments at your practice. Pet owners who have a strong relationship with their practice, or find the logistics of visiting a referral centre for frequent treatment difficult, often prefer this.
Chemotherapeutics that are well understood and commonly used are a good starting point for setting up chemotherapy in your practice.
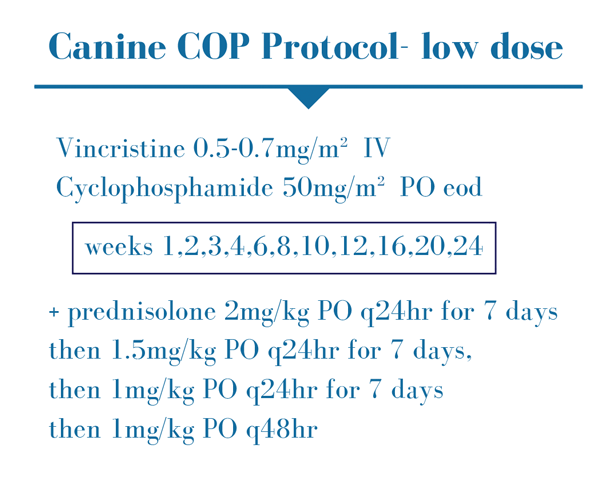
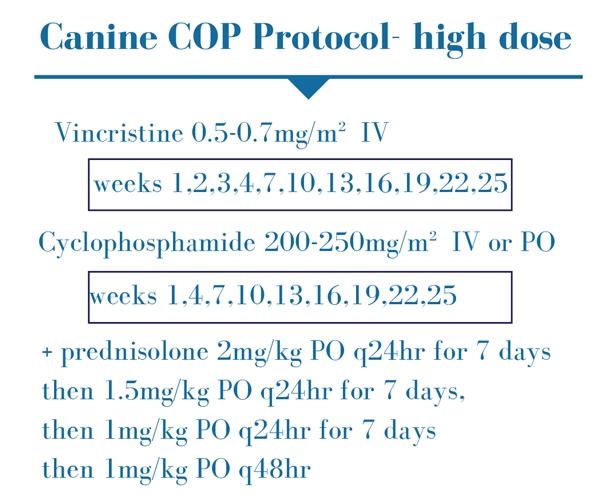
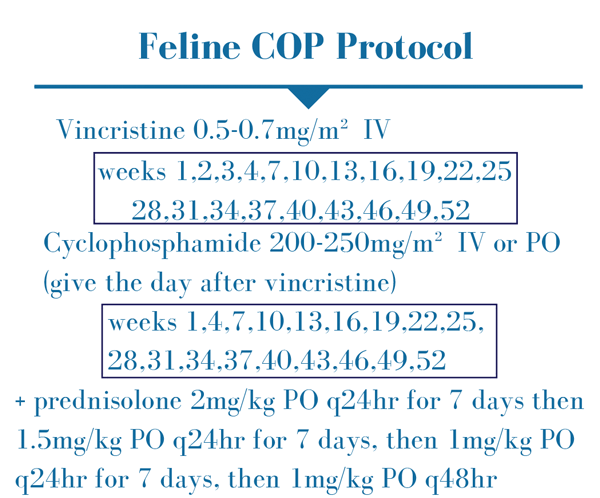
Vincristine and cyclophosphamide tend to be the most commonly used agents and are primarily used to treat dogs and cats with lymphoma. They are given in a cyclophosphamide, vincristine and prednisolone (COP) protocol (Figures 1 to 3) or combined with doxorubicin in a cyclophosphamide, doxorubicin, vincristine and prednisolone (CHOP) protocol (Figure 4). The latter tends to be associated with longer survival times in dogs1. The literature is less clear in cats, with one study reporting similar survival with a COP protocol to that reported with CHOP protocol2.
Administering doxorubicin requires more experience and is not commonly performed in general practice.

Intravenous chemotherapeutics, such as vincristine, require a “clean stick” IV catheter taped securely in place and checked for patency by alternately flushing (0.9 per cent NaCl) and drawing back blood (Figure 5).
If you have any doubts regarding patency of the IV catheter, remove it and try a different vein. Extravasation can have serious consequences, but is uncommon when care is taken (Figure 6).
Vincristine is given at a dose of 0.5mg/m2 to 0.7mg/m2. Erring on the side of caution while you become comfortable with these drugs and starting at the low end of the dose range is an option. You can always increase the dose at the next treatment if the first is well tolerated; we are aiming for the highest dose that maintains excellent quality of life.
Although all chemotherapeutics are myelosuppressive to some degree, the myelosuppressive effects of vincristine are generally mild. Haematology should be evaluated seven days after treatment. If neutrophils are less than 2×109/L at this point, delay treatment (if more is due). If neutrophils are less than 1×109/L, or if the patient is pyrexic, broad-spectrum antibiotics should also be used. If a treatment is delayed, consider further reducing vincristine dosage by 10 per cent to 20 per cent to avoid future delays.

Few patients experience gastrointestinal toxicity with vincristine. There is no evidence of this being reduced by maropitant premedication3. Prescribing oral maropitant at standard doses for the patient to have at home, if needed in the days after chemotherapy, is instead recommended. Gastrointestinal signs more than five days after chemotherapy are unlikely to be related to treatment.
Inappetence and vomiting can also result from ileus associated with vincristine. Ranitidine can help in these cases, again only if clinical signs occur.
If significant myelosuppressive or gastrointestinal adverse effects occur after vincristine, it is worth contacting a veterinary oncologist to discuss possible causes as this is not the norm. Genetic testing for abnormalities in drug metabolism may be recommended (for example, mutation of the multidrug resistance gene, MDR1).
Cyclophosphamide can be given orally or IV at 200mg/m2 to 250mg/m2, 4. Oral administration is simpler, but may require compounding to smaller capsules.

Gastrointestinal toxicity is uncommon after cyclophosphamide and it is not recommended to premedicate with antiemetics3. Myelosuppression is expected, but rarely severe. Testing haematology seven days after treatment is recommended and the advice for delaying chemotherapy is as for vincristine.
Cyclophosphamide can also cause sterile haemorrhagic cystitis. This is most likely to be due to accumulation of the irritant metabolite acrolein in the urine causing chronic inflammation. This adverse effect is not common, but the likelihood increases with cumulative dosing5.
Furosemide 2mg/kg IV or SC, used alongside cyclophosphamide, encourages evacuation of the irritant metabolites from the bladder6. Another option reported is furosemide 0.5mg/kg q12hr for two days at the time of cyclophosphamide administration7.
Using furosemide alongside cyclophosphamide is reported to reduce the incidence of sterile haemorrhagic cystitis from approximately 12% to close to 2%7. It is important to note furosemide will not be practical for low-dose COP protocols due to the frequency of dosing.
Dogs receiving any type of protocol containing cyclophosphamide should have frequent access to fresh water and the outdoors for urination to limit the amount of time the urotoxic metabolites are present in the bladder.
Furosemide is not given to cats receiving cyclophosphamide; this species is not prone to developing this side effect.
A third commonly used chemotherapeutic is vinblastine.

Vinblastine/prednisolone protocols remain the first line of treatment for many dogs with mast cell tumours (Figure 7). These are not straightforward with regard to prognostic indicators and when to administer chemotherapy so seek advice from a veterinary oncologist before making treatment recommendations.
If there is cause for vinblastine administration, the recommendations are akin to those of vincristine. The drugs are of the same class and behave similarly. The dose for vinblastine in dogs is 2mg/m2 IV.
Tyrosine kinase inhibitors (TKIs), such as toceranib and masitinib, are anti-cancer medications that can also be used in general practice.
These drugs are not the first line of treatment for mast cell tumours and can be expensive. However, they have the advantage of being administered orally, so can be useful in general practice.
Patients starting TKIs should have haematology, biochemistry, urine analysis and blood pressure tests before treatment and regularly throughout the treatment period to monitor for adverse effects. They tend to be well-tolerated medications, with gastrointestinal side effects the most common adverse issue.
When counselling owners about chemotherapy, the aforementioned side effects should be discussed. It’s important to emphasise these side effects are not common and are treatable when they occur.
Owners of dogs with continuously growing hair (non-shedding breeds) should be counselled about the likelihood of hair loss.
Chemotherapy can be stopped at any time if side effects affect quality of life, or the drugs in the protocol can be altered to improve quality of life. Owners often need to be assured treatment will not continue if it is not in the best interest of the patient.
Before administering chemotherapy, ensure you have an appropriate location to provide treatment without interruption. This location should be easy to clean and have emergency eye wash and shower facilities nearby.
Determine who may be willing to assist with treatment, with the understanding those who are pregnant or trying to conceive should not be involved in drug preparation, administration or cytotoxic patient nursing.
Buy personal protective equipment (gloves, gowns and masks) appropriate for chemotherapy. Ensure you have an appropriate waste disposal system for cytotoxic waste. Use signs to identify all areas where cytotoxics are prepared and used.
Ideally, buy disposable closed collection systems for safer administration8. If this is not possible, use a Luerlock system. Make sure you have a spill kit and a precautionary extravasation plan.
Drugs can be bought in ready-to-administer doses or prepared in a negative pressure isolator or biological safety cabinet if the former is not available.
No food or drink should be consumed in the preparation or administration area. Oral medications should not be split, crushed or otherwise manipulated.
All cytotoxic waste should be sealed in a zip-locked bag before depositing in a cytotoxic waste bin. Ensure you have an appropriate protocol for cleaning cytotoxic areas and clean regularly.
It is known small amounts of chemotherapy metabolites are present in the blood and excreta of patients receiving chemotherapy9,10. What is not well understood is whether these amounts are sufficient to harm humans.
Given the lack of information, it is prudent to take care handling chemotherapy patients. Label the cages of patients that have received chemotherapy and wear gloves when handling them. Ensure they are walked frequently to avoid contamination of their cage with urine or faeces containing chemotherapy metabolites and clean cages wearing personal protective equipment if contamination occurs.
Administering chemotherapy in general practice safely takes some preparation. Procedures should be more straightforward once protocols and facilities are established, but if you have any concerns or questions, don’t hesitate to contact a specialist.
Importantly, administer the treatment without time pressure if possible and find somewhere quiet for administration. It is generally easier with a calm, quiet patient – and reducing stress during administration is an important part of maintaining good quality of life for patients.