30 May 2016
Toby Gemmill and Bill Oxley discuss methods of assessing and diagnosing a common orthopaedic disorder that usually affects small breed dogs, and the treatment options available.

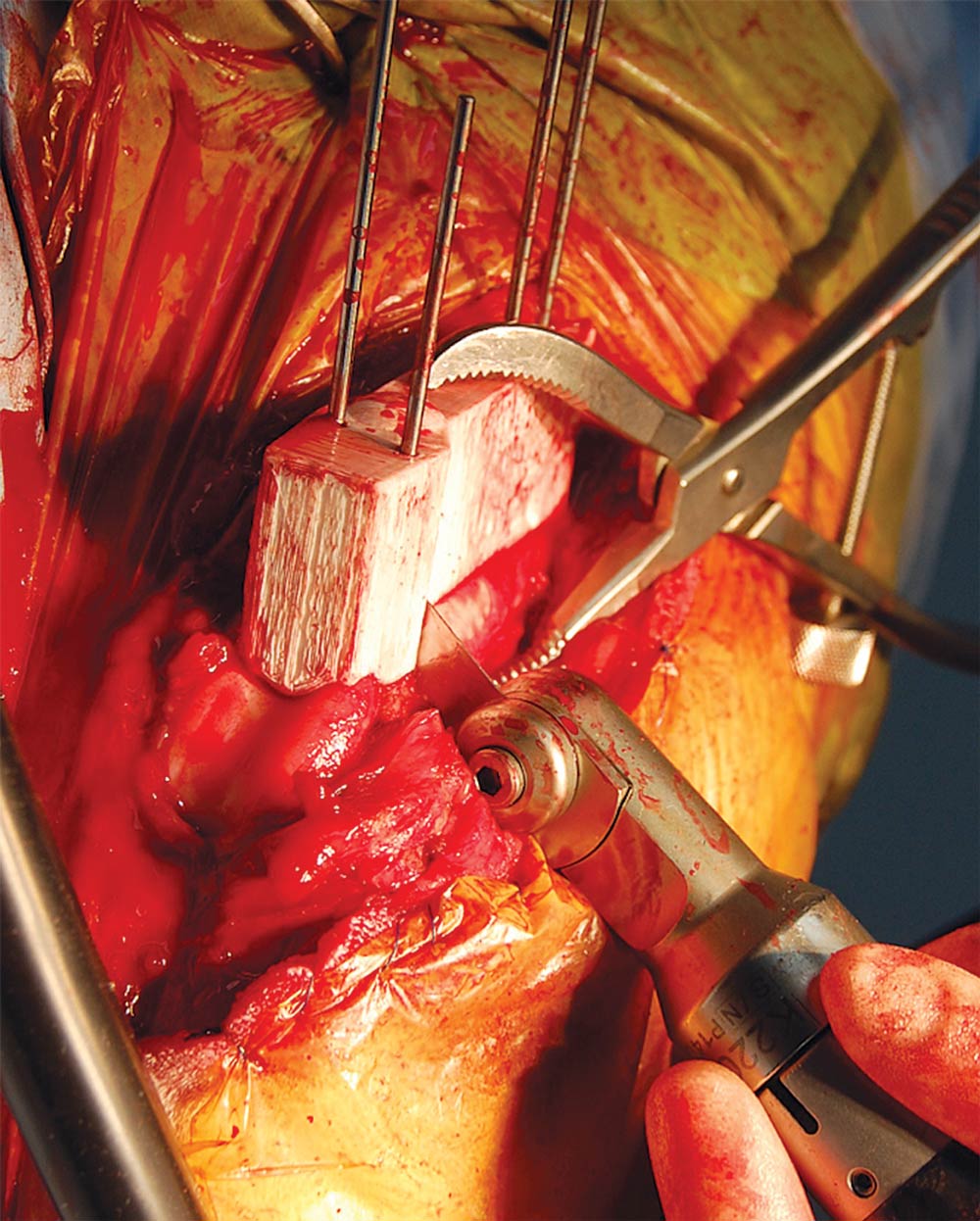
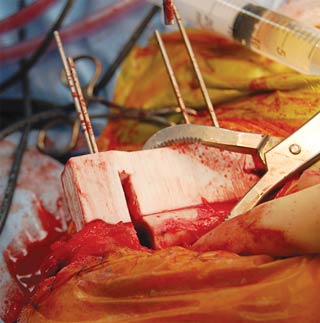
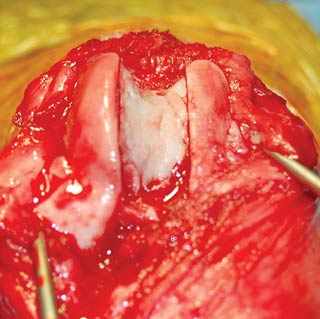
Figure 6b. The use of customised cutting and reduction guides to assist femoral osteotomy in a complex case. Intraoperative image showing the cutting guide attached to the cranial aspect of the femur with pins. The saw blade is positioned using the slot in the guide.
Medial patellar luxation (MPL) is a commonly encountered condition in small animal practice and can cause lameness, pain and secondary osteoarthritis.

Historically, the condition was seen more commonly in small breed dogs; however, increasing reports have existed of patellar luxation in larger breeds.
Yorkshire terriers, miniature poodles and cavalier King Charles spaniels are over-represented and, among large breeds, Labrador retrievers and mastiffs appear to be especially predisposed.
MPL is recognised more commonly than lateral patellar luxation. Although MPL has been described as a congenital condition, it is thought, in most cases, affected dogs are born with normal stifles and problems develop as they grow.
Clinical signs associated with MPL vary depending on the severity of the patellar instability, which can be quantified using a four point grading scheme (Table 1).
In most cases, grade one results in minimal clinical signs and can be treated conservatively; however, owners should be warned deterioration can occur, usually in association with other problems, such as cranial cruciate ligament deficiency or trauma to the stifle joint.
Dogs with a grade two are often presented with a history of an intermittent lameness. This can be relatively severe, although affected dogs can usually recover rapidly and walk normally once the patella is reduced.
Grade three will often lead to a more persistent lameness. It is important to differentiate this clinically from grade four, since this can affect prognosis following treatment. In most cases, dogs with grade two to grade four are surgical candidates. On occasions, however, some small breed dogs can cope surprisingly well without surgery and may be treated conservatively.
Medial patellar subluxation, where the patella rides on the medial trochlear ridge, is also occasionally encountered, especially in bulldogs and bull terriers, leading to the rapid development of femoropatellar osteoarthritis, and can be extremely debilitating.

Although MPL is often considered a disease of the patella, it has been recognised the pathogenesis relates to underlying deformities of the limb, leading to malalignment of the quadriceps mechanism with respect to the trochlear groove and consequential maltracking of the patella. Therefore, the patellar instability is effectively a clinical sign of the underlying deformity.
These deformities can vary in severity and complexity. Distal femoral varus deviation, external torsion of the femur and hypoplasia of the trochlear groove are common. Valgus deviation and torsional deformities of the tibia are also encountered concurrently in some cases, although tibial deformities are not thought to cause MPL per se.
Tibial deformities are often compensatory for femoral deformities. Although medial deviation of the tibial tuberosity is often described, it is thought, in most cases, this results from internal rotation of the tibia with respect to the femur rather than any bony deformity of the tibial crest.
The aim of MPL surgery is to stabilise the patella in the trochlear groove by restoration of quadricep alignment and appropriate patellar tracking, as well as deepening the trochlear groove, where appropriate. In addition, tension in regional soft tissues medial or lateral to the patella should be balanced, generally by medial desmotomy and lateral capsular and fascial imbrication.
Although the presence of underlying limb deformities has been recognised for many years, restoration of quadriceps alignment and patellar tracking has, historically, been achieved by surgery on the stifle itself, usually by means of tibial crest transposition. While this is an effective means of treatment and remains very useful in cases with internal tibial rotation, recurrence of patellar instability following tibial crest transposition is not uncommon, especially in cases with severe grade four MPL.
It has been suggested this relatively high recurrence rate could be due to a failure to recognise and directly address the underlying deformity of the limb. Indeed, in dogs where underlying femoral deformities were treated, the prognosis appeared to be improved, even in severely affected cases (Swiderski and Palmer, 2007; Roch and Gemmill, 2008).
These concerns have led to a reappraisal of the assessment and treatment of dogs with MPL.
Careful assessment of radiographs can allow identification and quantification of underlying deformities, particularly those involving the femur. This can allow correction of deformities using corrective osteotomies, where appropriate.
Unfortunately, because of the morphology of the femur, reliable quantification of femoral alignment can be challenging as minor errors in positioning can lead to significant errors in measurements. Therefore, perfectly positioned orthogonal projections of the femur are required.
From the caudocranial radiograph, the proximal anatomic femoral axis and distal joint reference line can be identified, and the anatomic lateral distal femoral angle (aLDFA) determined (Figure 1).
Normal ranges for the aLDFA have been determined for some breeds (Tomlinson et al, 2007); for normal Labrador retrievers this angle ranges from 94° to 100°. In most breeds, an osteotomy to realign the femur is considered when the aLDFA exceeds 100° to 102°, corresponding to a distal femoral varus deviation of greater than 10° to 12°.
It should be borne in mind if compensatory tibial deformities are also present, it may be necessary to correct these in some dogs.
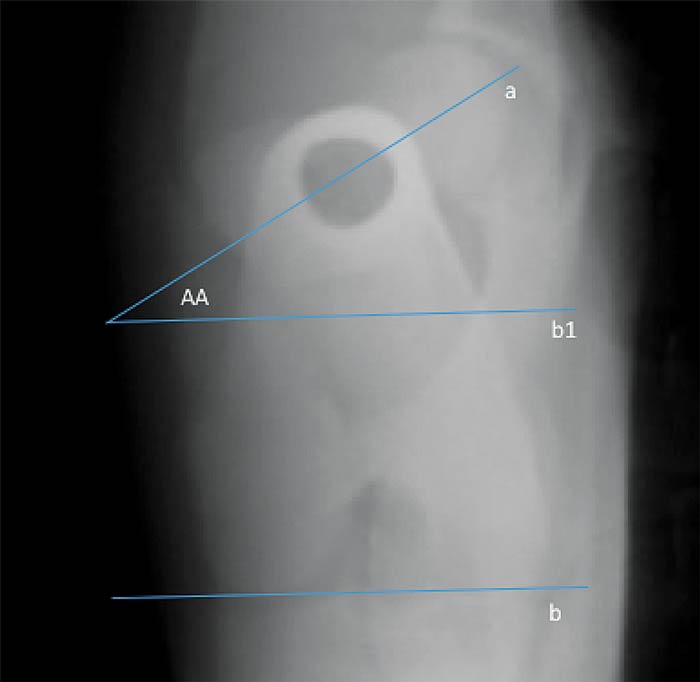
In addition to standard orthogonal radiographs, an axial proximodistal projection of the femur can be obtained to give an indication of femoral torsion (Figure 2). The angle of anteversion (AA) can be determined from the intersection between a line drawn along the femoral neck and another drawn along the caudal aspect of the femoral condyles. Assuming the hip joint and proximal femoral anatomy are normal, the AA should range from approximately 20° to 30°, although breed variations in this angle are poorly documented.
MPL is often associated with a low AA, corresponding to external femoral torsion. Where present, this can be corrected by femoral osteotomy.
Because of the challenge of obtaining perfectly positioned radiographs, CT is often used to assess femoral alignment. Following a standard CT scan of the pelvic limbs, 3D images can be created, which can be manipulated to produce perfect mediolateral, caudocranial and axial views of the femur to allow accurate assessment of femoral alignment. Measurements obtained from semi-transparent images (Figure 3) have been shown to be repeatable and highly precise (Oxley et al, 2013).
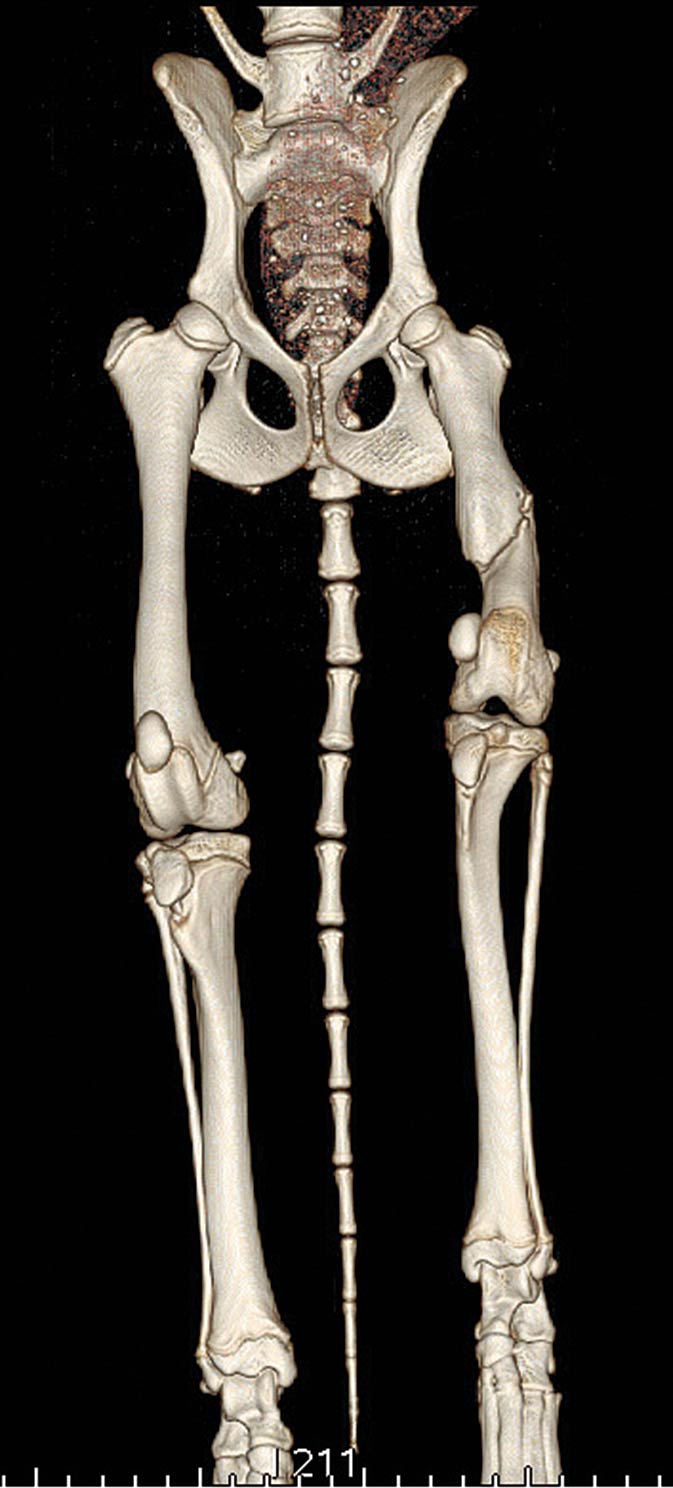
Surface rendered images (Figure 4) can be useful to assist in surgical planning. Images of the tibia can also be easily created, allowing assessment of any concurrent tibial deformities. In addition, CT scans using modern systems can be acquired very rapidly, reducing the sedation or anaesthetic time required to obtain a complete series of high quality radiographs.
Careful assessment of limb alignment prior to surgery allows detailed planning of surgical treatment in each case. Because the nature and severity of the deformities is highly variable, different surgical options are required in different cases. Selection of the most appropriate surgical options can be daunting; it can be helpful to make a list of all the deformities present and consider the need to correct each of these individually.
It is also important to bear in mind more complex procedures are often more expensive and carry a potentially greater risk of postoperative complications. In general terms, the simplest surgical options should be selected, provided appropriate quadriceps alignment and patellar tracking are restored.





The surgical technique for femoral osteotomy has evolved. In most cases, a lateral approach is made to the stifle joint and the distal femur. A jig is applied to the cranial aspect of the bone and either an opening or closing wedge osteotomy is performed using an oscillating saw, to allow correction of angular deformities.
Torsional deformities can also be addressed. Performing femoral osteotomy without the use of a jig is discouraged, since this can result in inadvertent torsional malalignment. Following reduction, the osteotomy is stabilised using one or two bone plates and screws. Locking systems are preferred, if available (Figure 5).
In more complex cases, 3D printing of affected bones can greatly assist surgical planning. In addition, using computer modelling, osteotomies can be performed electronically allowing printing of a second “post-correction” bone model. This allows bone plates to be precontoured to the shape of the bone prior to surgery, which facilitates accurate osteotomy reduction and decreases surgical time. 3D printing can also be used to create custom osteotomy and reduction guides (Figure 6).
The osteotomy guide is applied to the bone using pins; this facilitates creation of an accurate osteotomy. The osteotomy guide is removed, but the pins are left in place. The reduction guide is slid on to the pins, reducing the osteotomy and restoring bone alignment. The device also maintains reduction of the osteotomy while precontoured plates are applied.
As well as restoring quadriceps alignment and patellar tracking by correction of underlying deformities or performance of a tibial crest transposition, it is necessary to deepen the trochlear groove in many cases.
The decision to perform a trochleoplasty is subjective, but should be considered if the depth of trochlear groove is less than 30% to 50% the craniocaudal height of the patella, as measured from a mediolateral radiograph of the stifle. V-recession sulcoplasty has been performed for several years and allows preservation of the articular surface of the trochlear groove, at least in its central region.
Rectangular block recession sulcoplasty starts at the apex of the trochlear ridges, slightly converging osteotomies are performed in a craniolateral to caudomedial direction. An osteotome is used to remove an osteochondral block from the trochlear groove. Additional bone is removed from the resultant femoral defect before the block is replaced in a recessed position (Johnson et al, 2001; Figure 7).


Another possibility developed is augmentation of the trochlear ridges using a poly-
ethylene insert. However, peer-reviewed evidence of efficacy is lacking. Complete replacement of the trochlear groove has also been described. This is useful for cases with complete absence of the trochlear groove or severe derangement of the femoropatellar joint, often seen with chronic medial patellar subluxation.

A frontal plane osteotomy is performed and the entire cranial aspect of the distal femur resected. A base plate is secured to the femur using screws and the patellar groove replacement (PGR) clipped into place (Figure 8). The PGR is highly polished with a diamond-like coating, giving a very low coefficient of friction. This device has been shown to be successful in the management of challenging MPL cases (Dokic et al, 2015).
It is also possible to change the orientation of the frontal plane femoral osteotomy or the precise position of the PGR to address certain femoral angular or torsional deformities and improve quadriceps alignment. While PGR is a promising development and postoperative complications appear to be low, the advantages must be weighed against the possibility for catastrophic complications.
These developments have led to improved outcomes following surgery to treat MPL; in particular, the risk of recurrence of patellar instability appears to be reduced. However, decision-making in individual cases can be challenging. It is recommended full assessment of limb alignment and bony anatomy, using high-quality radiography or CT, is performed in all cases.
Surgery should be planned on an individual basis, aiming to restore quadriceps alignment and patellar tracking in all cases, as well as ensuring adequate depth of the trochlear groove and balancing the soft tissues. To minimise the potential risk of postoperative complications, the simplest surgical techniques allowing these aims to be achieved are selected.
In many dogs, conventional tibial crest transposition can be performed; however, femoral and occasionally concurrent tibial corrective osteotomies should be considered for more complex cases.
Case assessment and novel techniques for management of medial patellar luxation will be covered in detail in the forthcoming AOVET course on “Advanced pelvic limb osteotomy”, chaired by one of the authors, planned for 17 to 19 May 2017 at the Royal College of Surgeons in Edinburgh.