28 Mar 2022
Quentin Fournier DVM, DipECVIM-CA(Oncology), MRCVS shares a case study where advanced ultrasound technology provided the basis for a successful procedure.
Quentin Fournier
Job Title
Figure 1a. Plato’s body map, indicating the location of his mast cell tumour. From our previous work, the left medial iliac lymph node (5, draining blue area) and/or the left inguinal lymph node (6, draining yellow area) were the most likely lymph nodes to be draining Plato’s mast cell tumour.
Plato is an affectionate and loved nine-year-old, male, neutered pug that was presented to Fitzpatrick Referrals for management of a SC mast cell tumour (MCT) on his left flank.

The family noted this 2.5cm soft and well-defined mass about four weeks prior to referral, and it had been very stable in size and appearance since.
Only 4% of SC MCTs have originally been reported to metastasise, but this may be underestimated, as in our experience the incidence of metastasis is higher when thorough lymph node (LN) assessment (of the appropriate LN) is performed.
Following the recommendations of the author, senior clinician in medical oncology, contrast-enhanced ultrasound sentinel LN mapping was performed to identify precisely which LNs were draining his tumour.
Anatomically, either the left medial iliac or left inguinal LNs could be potentially draining the MCT, but this is difficult or impossible to predict in advance (Figures 1a and 1b).
Identifying the correct draining LN, however, helps families and the oncology team make decisions based on the most accurate information on Plato’s specific situation – namely individualised cancer care.
Around the nodule, we injected a contrast agent consisting of a liquid containing microscopic bubbles of gas, harmless and eliminated from the tissues within minutes.
Special advanced ultrasound allowed our radiologist to visualise the contrast real-time, travelling in the lymphatics and first accumulating in the left inguinal LN (in the groin), and after a few minutes also in the left medial iliac LN (inside the abdomen).
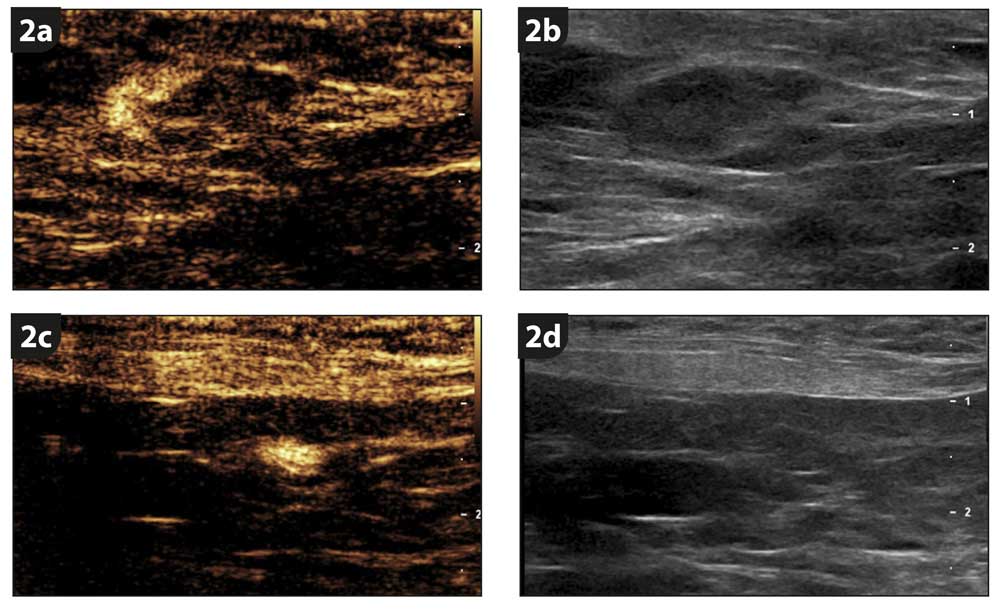
The left inguinal LN was moderately enlarged (7mm) with a second, small 2.5mm one, while the left medial iliac LN was within normal limits and too small to be sampled (Figure 2). A fine-needle aspirate of the left inguinal LN unfortunately confirmed it was metastatic, but the liver and spleen were free of mast cells.
A week later, the SC MCT was removed at surgery with wide margins. Initially hesitant to remove the left medial iliac LN, as it was a normal size and within the abdomen, given we could directly follow the microbubbles from the tumour to the internal node, the family elected to remove it under the same anaesthetic rather than perhaps need a second surgery in the future.
Plato recovered well from his procedure. Histological analysis confirmed his MCT to be completely excised, but all LNs removed showed evidence of early metastasis.
Based on the current scientific data, only 3% of SC MCTs with a benign appearance and low proliferation index metastasise, but with new techniques we are learning the risk is likely higher, and we are very happy that Plato’s family followed our recommendations and all affected LNs were removed with one procedure.
Several publications suggest that removing a metastatic LN likely carries a therapeutic benefit, so we remain optimistic for Plato’s future. Given the early signs of spread, Plato underwent a three-month course of vinblastine/prednisolone chemotherapy protocol to reduce the risk of relapse.
Plato remains cancer-free a year after his diagnosis, has needed no further surgery, and we wish him a long and happy life.
Contrast-enhanced ultrasound sentinel LN mapping is only available in a few places in Europe, and it allowed us to accurately identify the draining LNs, even when internally, and remove the metastatic LNs in a single procedure.
This would likely not have been possible otherwise, and cancer spread would have been left behind. This is a very good illustration of the medical oncologists, radiologists and surgical oncologists at Fitzpatrick Referrals Oncology and Soft Tissue, adapting state-of-the-art human techniques in cancer care to offer the best possible management and outcome for animals.
This article has been adapted from Fournier Q, Thierry F, Longo M et al (2021). Contrast-enhanced ultrasound for sentinel lymph node identification in the routine staging of canine mast cell tumours: a feasibility study, Veterinary and Comparative Oncology 19(3): 451-462.