24 Sept 2024
Kayal Patel shares some of the most common types and causes of these lesions, and how to treat them.
Kayal Patel
Job Title
Figure 1 (main). Use of slit beam on direct ophthalmoscope allows accurate assessment of ulcer depth.
The cornea serves as the eye’s primary optical surface, playing a crucial role in refracting light while also acting as a protective barrier between the eye and the external environment.
For optimal light refraction, and to ensure that sufficient light reaches the retina to form clear images, maintaining corneal transparency is essential. This transparency is facilitated by several anatomical and physiological features, such as the absence of pigmentation and blood vessels, low cellular density, partial dehydration (known as “deturgescence”) and the precise arrangement of stromal collagen fibres.
Structurally, the cornea is composed of four distinct layers: epithelium, stroma, Descemet’s membrane and endothelium.
● Corneal epithelium: the corneal epithelium is a stratified, squamous, non-keratinised layer composed of five to seven cell layers. This layer undergoes continuous cell turnover, with surface cells regularly shed and replaced by new cells from the basal layer. Its primary functions are to anchor the tear film to the cornea and serve as a protective barrier against tears and external contaminants.
● Corneal stroma: the stroma is composed of keratinocytes, collagen and glycosaminoglycans, and makes up 90% of the corneal thickness. Its principal function is to provide mechanical strength to the cornea, maintaining its shape and structural integrity.
● Descemet’s membrane: Descemet’s membrane is the basement membrane of the endothelium and lies between the posterior stroma and the endothelium. In cases of severe corneal ulcers with full stromal loss, this membrane can become exposed, leading to a condition known as a “descemetocele.”
● Corneal endothelium: the corneal endothelium is a single layer of cells situated on the innermost part of the cornea, posterior to Descemet’s membrane. Its key role is to maintain corneal dehydration by actively pumping ions from the cornea into the aqueous humour, which is essential for corneal transparency.
Clinical signs of corneal ulceration include blepharospasm, epiphora, protrusion of the third eyelid and an increased blink rate.
It is essential to perform a complete ophthalmic examination on all patients presenting with ocular concerns. This examination should follow a structured approach, beginning with a hands-off assessment of the patient.
The next step is to conduct a Schirmer tear test (STT) by placing the test strip in the lateral aspect of the inferior eyelid. In cats, normal STT values vary, but a study of 120 normal cats reported a median value of 18mm per minute, with a range of 9mm to 34mm1.
A neuro-ophthalmic examination should also be performed, including assessments of the menace response, pupillary light reflex, palpebral reflex and dazzle reflex. Following this, intraocular pressure should be measured before proceeding with a close direct examination. This examination should be conducted in a dark environment using either a direct ophthalmoscope or a slit lamp biomicroscope. The slit feature is particularly useful for obtaining a cross-sectional view of the cornea, which allows for an accurate assessment of ulcer depth (Figure 1).
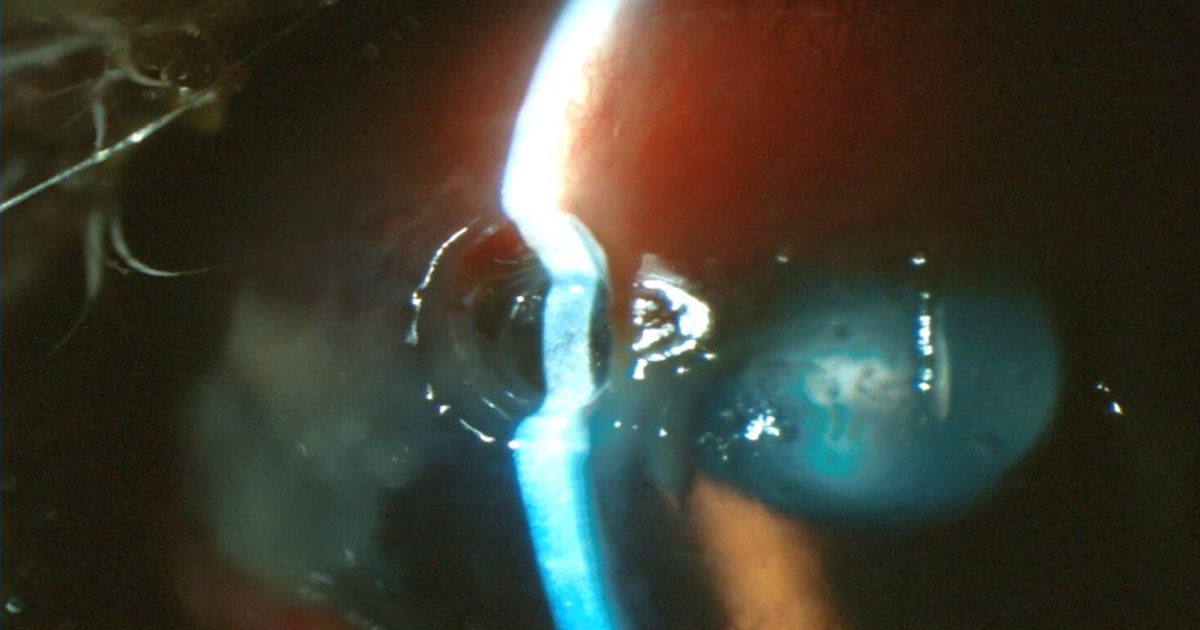
Figure 1. Use of slit beam on direct ophthalmoscope allows accurate assessment of ulcer depth.
If a direct ophthalmoscope is not available, a focal light source and condensing lens can be used to examine the retina.
Finally, the cornea should be stained with fluorescein to aid in the diagnosis of corneal ulcers. Fluorescein is hydrophilic and will adhere to any exposed corneal stroma, but it will not bind to the hydrophobic corneal epithelium or Descemet’s membrane. When using a fluorescein strip, it is important to apply it to the conjunctiva to avoid causing iatrogenic corneal erosion. After applying the fluorescein stain, the eye should be thoroughly flushed before examination with cobalt blue light.
In feline patients, superficial ulceration should generally be presumed to result from feline herpes virus unless proven otherwise.
While other causes such as eyelid abnormalities (such as entropion, ectropion, agenesis, dermoid or neoplasia), tear film deficiencies, eyelash abnormalities (such as ectopic cilia or trichiasis) or neurological conditions (such as trigeminal nerve paralysis or facial nerve paralysis) can also lead to ulceration, these are less common in cats2.
Any identified abnormalities should be carefully evaluated alongside the clinical signs to determine whether they are the primary contributors to the ulceration.
Feline herpes virus type 1 (FHV-1) is a highly contagious alpha-herpes virus that affects cats globally. This DNA virus is characterised by its rapid replication within epithelial cells, lifelong latency within neural cells and strict host specificity to cats.
Transmission occurs primarily through direct contact with virus-containing droplets from oral, nasal and conjunctival secretions of infected cats. The virus is widespread, with an estimated 75% to 97% of the global cat population being seropositive.
Upon infection, FHV-1 predominantly replicates in the epithelial cells of the conjunctiva, nasal mucosa and tonsils. The process of viral replication results in the lysis of these epithelial cells, leading to erosions and ulcers on the mucosal surfaces.
A portion of the virus also travels along the neural axons, establishing lifelong latency in the trigeminal ganglion. During this latent phase, the virus remains dormant, and the infected cat shows no clinical signs. It is estimated around 80% of infected cats become chronic carriers of FHV-1.
Reactivation of the virus, known as recrudescence, occurs in approximately 40% of these carriers, often triggered by stress. During recrudescence, the virus resumes replication, potentially leading to the reappearance of clinical signs.
Factors that can trigger reactivation include the following.
● Endogenous factors: underlying conditions, such as FIV, FeLV or physiological stressors such as lactation.
● Exogenous factors: environmental changes such as the introduction of new cats into the household or a stay in a cattery.
● Iatrogenic factors: medical interventions, such as the use of systemic or topical steroids.
Understanding the nature of FHV-1, its transmission and the factors that contribute to viral reactivation is crucial for managing this common feline infection.
Ophthalmia neonatorum
If feline herpes virus infection occurs before a kitten’s eyelids open, significant inflammatory debris can accumulate within the conjunctival sac, leading to a condition known as ophthalmia neonatorum. Early recognition and treatment are crucial to prevent long-term ocular damage.
Conjunctivitis
During the initial phase of rapid viral replication or upon reactivation of FHV-1, lysis of epithelial cells can result in conjunctivitis. This condition is often one of the first clinical signs, characterised by redness and swelling of the conjunctiva, and mucopurulent discharge from the eyes.
Ulcerative keratitis
● Herpetic ulcers: these ulcers typically involve the loss of corneal epithelium without stromal involvement. If the stroma is affected, it often indicates additional factors such as opportunistic bacterial or fungal infections adhering to the compromised tissue.
● Dendritic ulcerative keratitis: dendritic ulcers are considered pathognomonic for FHV-1 infection. However, they are rarely observed as such because these branching lesions quickly evolve into larger geographic ulcers. The precise mechanism behind the formation of dendritic ulcers remains unclear (Figure 2).
● Indolent ulcers (Figure 3): these chronic, superficial ulcers are characterised by loose, non-adherent epithelium, resembling (but with very different pathogenesis) superficial chronic corneal epithelial defects as seen in dogs, and are frequently associated with FHV-1. Potential complications of untreated indolent ulcers include stromal keratitis and corneal sequestrum.
Corneal involvement: FHV-1 can affect the corneal epithelium, stroma or both, leading to a variety of clinical presentations. The degree of corneal involvement dictates the severity and type of ulceration.
Stromal keratitis
Stromal keratitis is thought to occur when viral antigens penetrate the corneal stroma, triggering an exaggerated immune response.
This immune-mediated reaction results in a range of clinical signs, including corneal stromal fibrosis, oedema, infiltration of white blood cells and vascularisation beneath an intact epithelium (Figure 4).
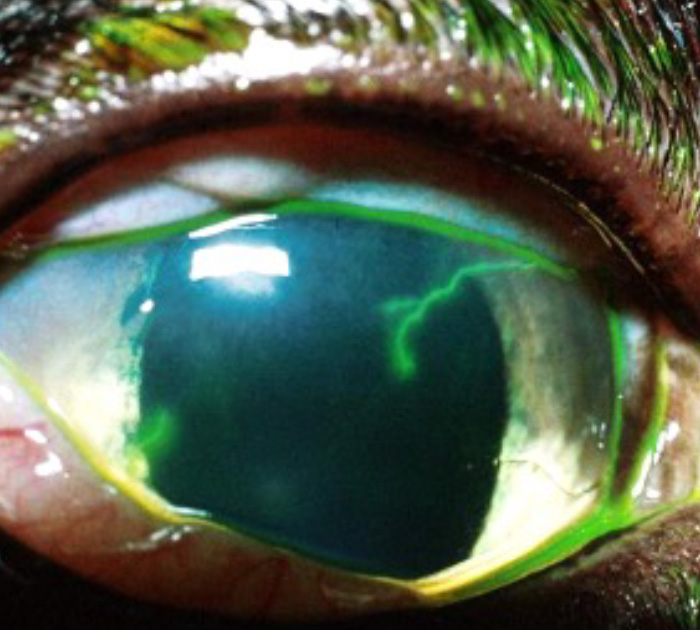
Figure 2. Dendritic ulcerative keratitis.

Figure 3. Indolent corneal ulcer.

Figure 4. Stromal keratitis.
Ulcerative keratitis
● Address underlying stressors: reducing environmental and physiological stressors can help mitigate flare-ups.
● Antiviral therapy: topical antiviral treatment, such as ganciclovir, administered at least four times daily, or systemic antiviral agents, such as famciclovir, is recommended.
● Symptomatic treatment: supportive care includes the use of topical tear substitutes, cycloplegics (such as cyclopentolate or atropine), topical antibiotics, such as chloramphenicol, and systemic NSAIDs to manage reflex anterior uveitis.
Indolent ulcers
● Debridement: gentle debridement with a cotton-tipped applicator under local anaesthesia (such as proxymetacaine) can help remove loose epithelium.
● Topical antibiotics: use broad-spectrum antibiotics such as chloramphenicol to prevent secondary bacterial infections.
● Cycloplegics: agents such as cyclopentolate or atropine are beneficial for pain relief and reducing ciliary body spasm.
● Concurrent antiviral therapy: topical antiviral treatment, such as ganciclovir, administered at least four times daily, or systemic antiviral agents, such as famciclovir, is recommended.
● Surgical intervention: if ulcers do not heal despite medical treatment, a superficial keratectomy should be considered.
● While diamond burr debridement has been documented in cats3, in the author’s team’s experience, gentle cotton bud debridement is extremely effective at eliminating the viral load from the affected epithelium, which combined with the previously outlined medical treatment, leads to successful healing of the ulcers.
Stromal keratitis
● Topical NSAIDs: NSAIDs such as flurbiprofen, ketorolac trometamol, or bromfenac can be used to reduce inflammation.
● Antiviral therapy: topical (ganciclovir) or systemic (famciclovir) antiviral agents are necessary.
● Immunomodulation: topical ciclosporin can be used to modulate the local immune response and prevent further stromal damage.
Overview
Stromal ulcers occur when ulcerative keratitis extends into the corneal stroma, typically due to a secondary microbial infection that triggers stromal destruction.
Clinical signs
A visible defect in the corneal surface, often described as a “crater effect,” is indicative of stromal involvement (Figure 1).
Diagnostic approach
Cytology and culture and sensitivity testing are essential to identify the underlying cause and guide treatment.
Classification
Stromal ulcers can be classified as either non-progressive or progressive.
● Non-progressive ulcers: these can often be managed medically. Treatment should be tailored based on the results of culture and sensitivity testing.
● Progressive ulcers: these are potentially vision and globe-threatening, and require aggressive treatment. Management typically involves intensive treatment with topical antibiotics, mydriatics/cycloplegics (such as cyclopentolate or atropine) and anti-proteolytic agents (Matrix metalloproteinases [MMPs] inhibitors – doxycycline/oxytetracycline, N-acetyl-cysteine [NAC], disodium-ethylene-diaminetetra-acetic acid [EDTA], ilomostast; combined MMP and serine proteinase inhibitor – serum, plasma)4.
Surgical intervention
If a stromal ulcer is rapidly progressive, involving more than 50% of the corneal thickness, or does not respond to medical therapy, surgical repair may be necessary.

Surgical consideration
Surgery is recommended for deep stromal ulcers, descemetoceles and full-thickness perforations – especially those with or without iris prolapse.
Severity and indication for surgery
Deep corneal ulcers can threaten both vision and the integrity of the eye.
Surgical intervention is often necessary when the lesion involves more than 50% of the corneal thickness or extends deeper (Figure 5).
Grafting techniques
A range of corneal grafting procedures have been successfully employed, including corneoconjunctival transposition, amniotic membrane grafts (Figure 6), autologous or heterologous corneal grafts, and synthetic or bioengineered grafts (such as those by BioSIS or BioCorneaVet; Figure 7).
Prompt referral of deep corneal ulcers is vital in improving outcome.

Figure 6. Amniotic membrane graft.
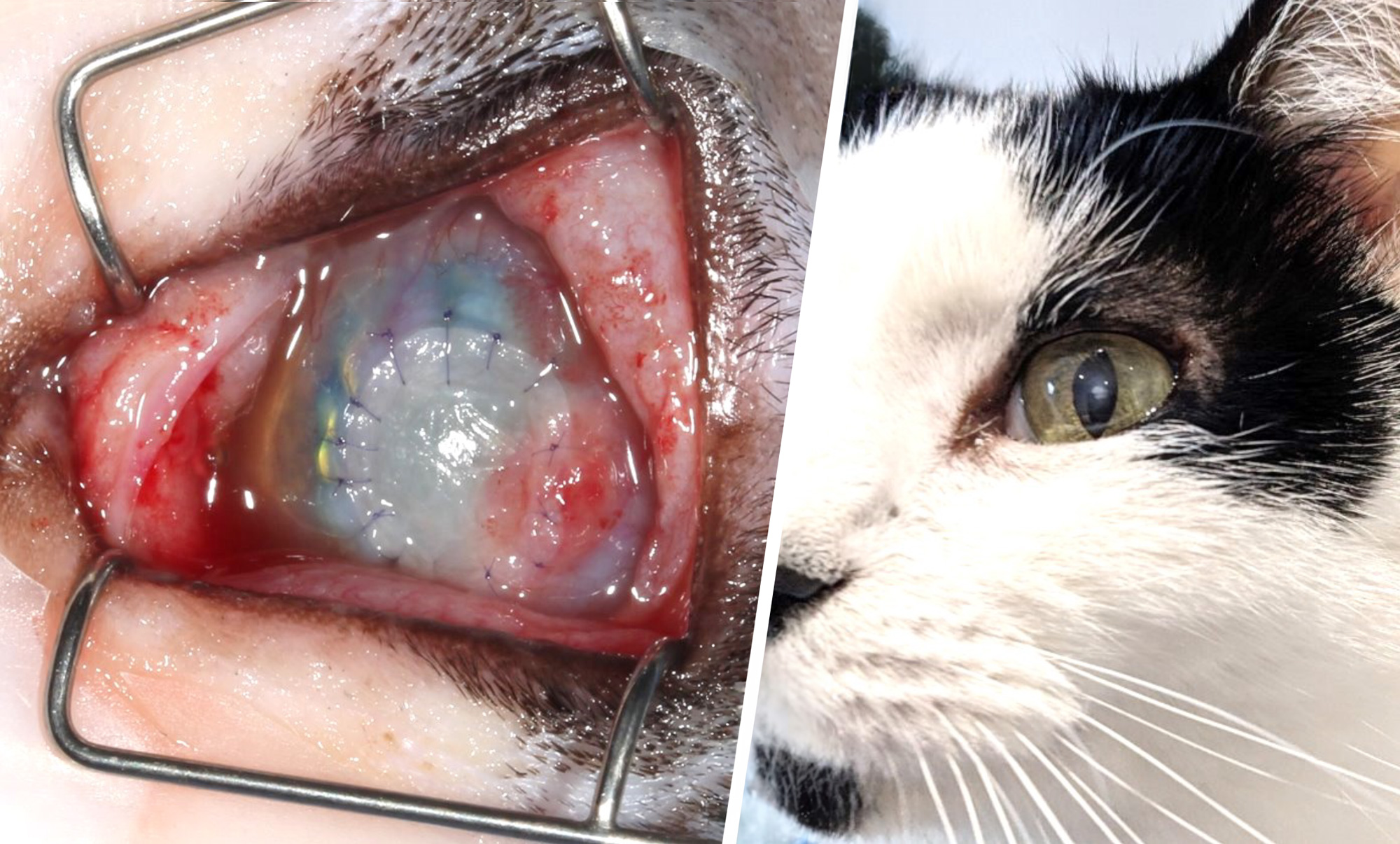
Figure 7. VetBiosis graft.
● Use of some of the drugs in this article is under the veterinary medicine cascade.