8 Aug 2016
Katherine Clarke
Job Title
Your first case of the morning is Jack, a five-year-old Manchester terrier that has been presented for a second opinion. He is lethargic, depressed and anorexic.
The main abnormality identified on clinical examination is dullness of thoracic percussion and muffling of respiratory noise in the ventral aspect of the lung fields bilaterally. Jack is otherwise in good condition (five out of nine) and clinical examination, including cardiac auscultation, reveals no further abnormalities.
Thoracic radiographs confirm the clinical suspicion of a pleural effusion. Ultrasound-guided thoracentesis yields a true transudate: protein 10g/l (reference range less than 25g/l), very low numbers of nucleated cells, predominantly macrophages, small lymphocytes and lower numbers of non-degenerate neutrophils.
Abdominal ultrasound is unremarkable apart from slightly reduced corticomedullary differentiation in both kidneys and a small volume of ascites.
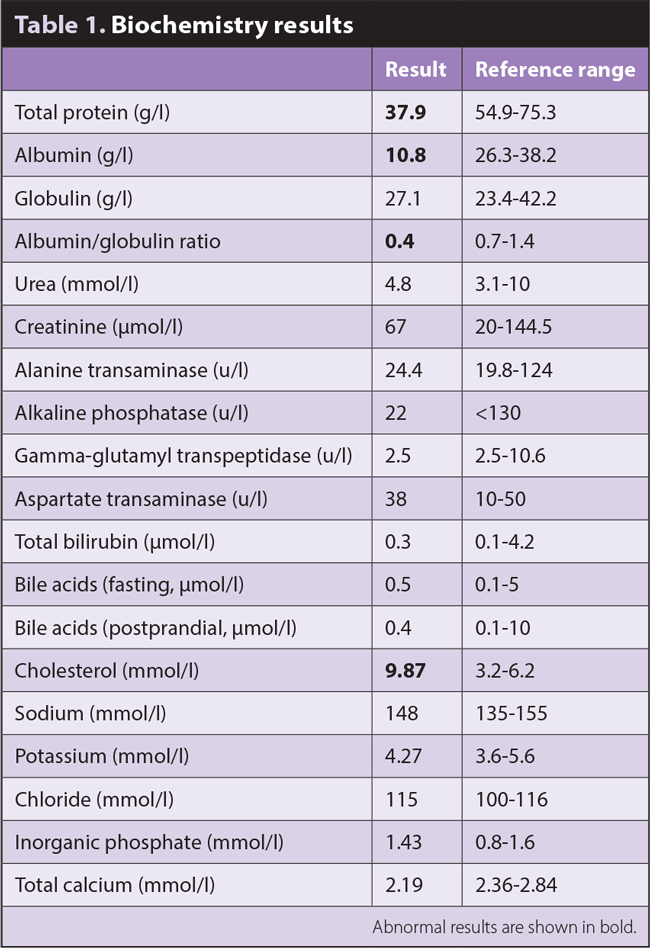
Haematology is unremarkable; the biochemistry results are shown in Table 1.
What are the main differential diagnoses?
The most significant findings are marked hypoalbuminaemia and hypercholesterolaemia. Once serum albumin falls below about 14g/l, effusions into thoracic and/or abdominal cavities can occur and would explain the pure transudate identified in Jack’s thorax. Although not present here, peripheral oedema can also occur.
Hypoalbuminaemia can be caused by:
Hypercholesterolaemia and an elevated urine protein ratio are also commonly seen and collectively known as nephrotic syndrome.
A urine sample, obtained from Jack via cystocentesis, was culture negative and had a urine protein:creatinine ratio (UPC) of 10.9 (reference range less than 0.5), confirming the presence of significant proteinuria – and, hence, a PLN.
Glomerular disease (such as glomerulonephritis) is suspected when the UPC is greater than 2 and can be triggered by any infectious, inflammatory or neoplastic disease.
A renal biopsy may be performed to identify the presence of an underlying immune-mediated disease and, therefore, these patients would benefit from immunosuppressive therapy. If biopsies are taken, it is vital they are sent for interpretation by a nephropathologist. The centre of choice is the Veterinary Pathology Diagnostic Centre at Utrecht University, the Netherlands.
Non-immunosuppressive medical treatment otherwise consists of an angiotensin-converting enzyme inhibitor – such as benazepril – aspirin, a renal diet and fatty acid supplementation.
Jack is a month into treatment, his serum albumin is normal and he is clinically very well.