5 Dec 2016
Jon Hardy introduces us to Stanley, and his two-week history of pruritus, alopecia and erythema, in the latest Case Notes.
Jon Hardy
Job Title
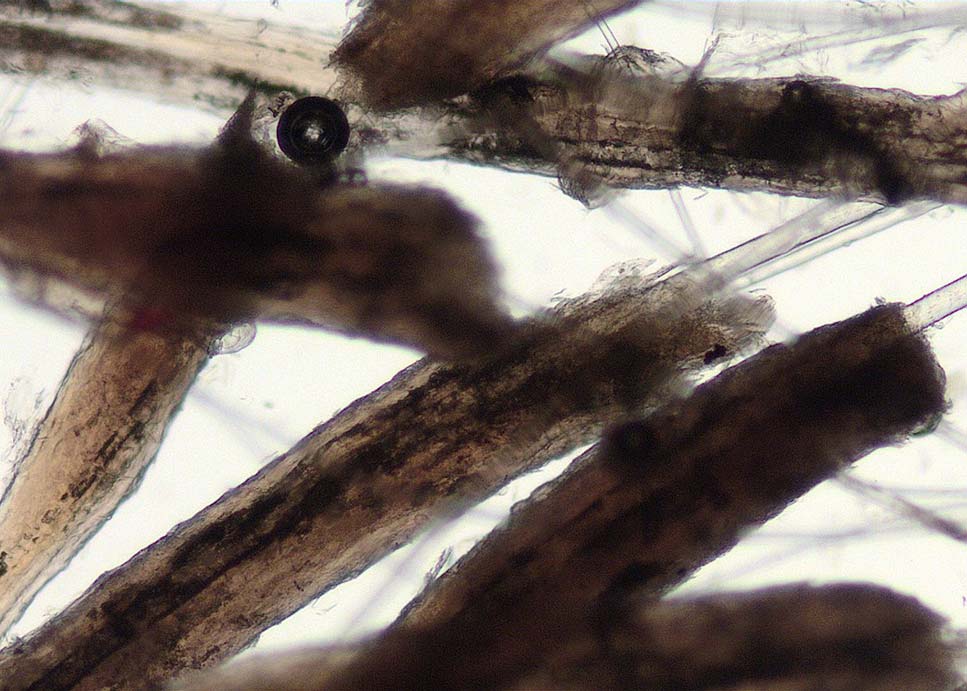
Figure 1. Hairs with adherent keratin and follicular material in a case of demodicosis.
Your first case of the afternoon is Stanley, a one-year-old male entire English bulldog with a two-week history of pruritus, alopecia and erythema. His owners are concerned as his littermates have been diagnosed with demodicosis.
You perform a general physical examination and find no significant abnormalities. Dermatological examination reveals an area of erythematous moist dermatitis on the distal left forelimb overlying the carpus. Multifocal areas of erythema and alopecia also exist throughout the coat, including the face and feet. Within these alopecic areas, you see keratinous material attached to the hair shafts.
Knowing demodicosis needs to be ruled out, you perform multiple deep skin scrapings from a range of affected sites. However, despite an extensive search, no parasites are found. You start to think of other differential diagnoses for pruritus and perform a coat brushing, flea combing, Wood’s lamp examination and tape impression, but nothing is found.


What do you do next?
Stanley’s signalment and the distribution of his lesions are certainly consistent with juvenile onset generalised demodicosis. The adherent keratinous material attached to the hair shafts, known as follicular casting (Figures 1 and 2), is also suggestive of this disease.
In some cases, particularly when considerable hair is present, performing effective skin scrapes can be difficult. These can be used as well. Hair plucks are performed by plucking small groups of hairs with fingers or forceps and placing them on to a microscope slide in paraffin oil (Figure 3). A coverslip is applied and the hairs are examined with low power microscopy (×4 or ×10 lenses; Figure 4).

Hair plucks are a very effective way of diagnosing demodicosis and, in most patients, are usually easier to perform than skin scrapings. They are also potentially safer to perform at sites such as the face and feet, and clipping of the hair is not necessary.
If follicular casting is present, these hairs should be chosen for sampling. A further option for diagnosis involves the microscopic examination of surface exudate, sometimes performed with prior squeezing of the skin1,2. This has been shown to have a diagnostic sensitivity similar to skin scrapings.
Although hair plucks are a very valuable diagnostic test, one paper found the diagnostic sensitivity to be lower than that for deep skin scrapings2. As such, it is advisable to perform both skin scrapings and hair plucks before ruling demodicosis out.