7 Aug 2017
Katherine Clarke discusses the clinical examination and blood results for an 11-year-old cocker spaniel with worsening haematuria.
Katherine Clarke
Job Title
Image © Argus / Fotolia
On a rainy Tuesday morning, you see an 11-year-old neutered male cocker spaniel with a 48-hour history of worsening haematuria.
The owners report he has become progressively weak overnight and has started passing fresh, clotted blood from his penis.
On physical examination, he is collapsed, mucous membranes are pale and tacky, capillary refill time is two seconds and petechiae are present.
He is tachycardic, with a heart rate of 160bpm, and his peripheral pulses are bounding. Fresh blood is dripping from his penis. Ecchymosis and petechiae are abundant on his ventral abdomen and thorax.
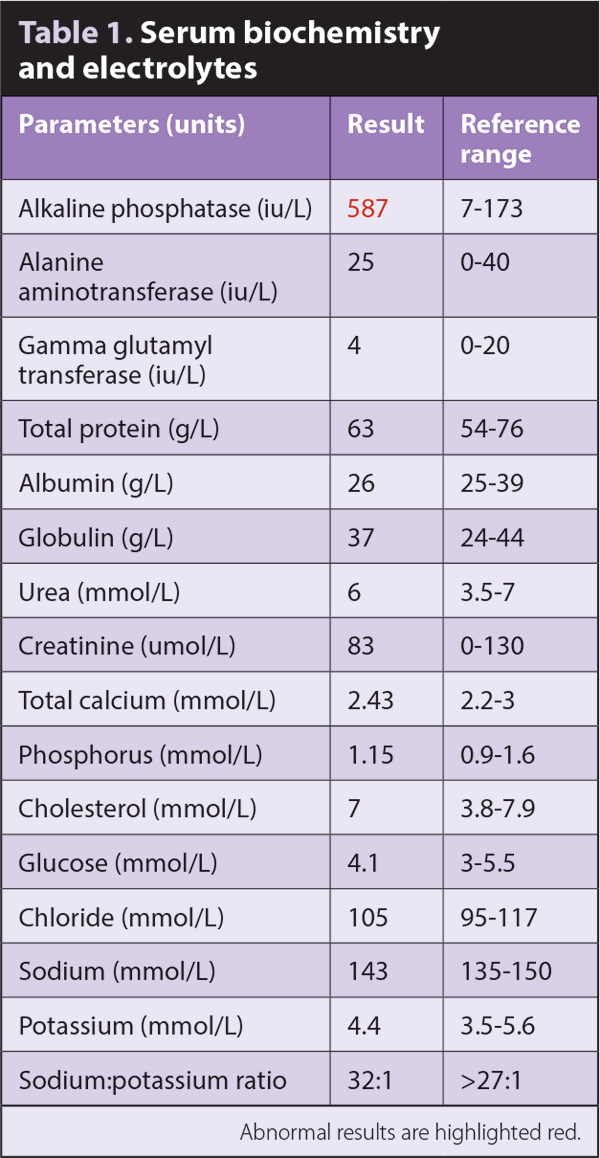
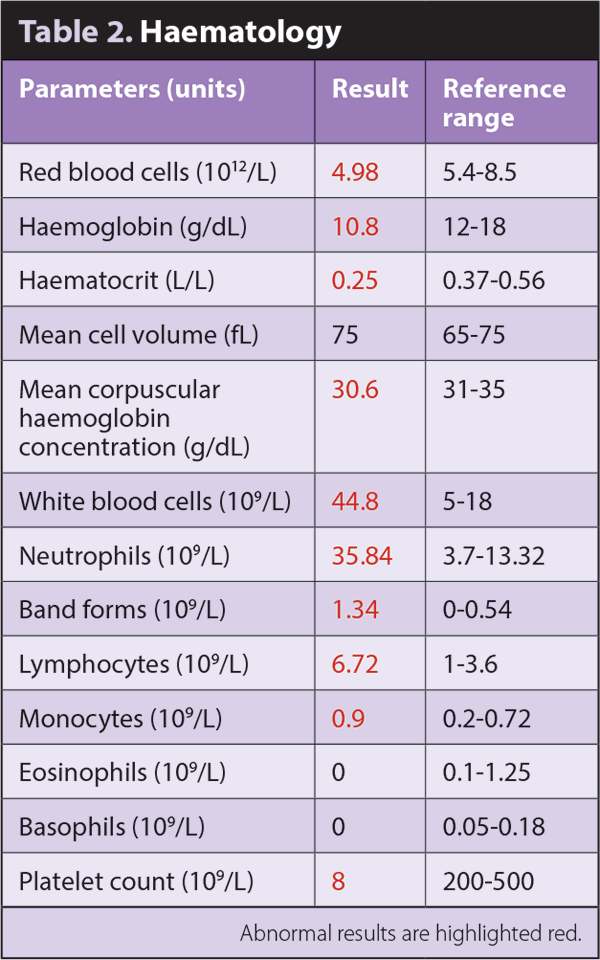
Biochemistry/electrolytes (Table 1) and haematology (Table 2) tests were performed. Abnormal results are highlighted red. On blood smear, platelets appear markedly reduced, with no reticulocytes seen.
Describe the biochemical and haematological abnormalities.
Haematology shows mild, normocytic, hypochromic, non-regenerative or pre-regenerative anaemia. A marked thrombocytopenia is present, confirmed on smear examination. A leukocytosis exists – consisting of a moderate lymphocytosis and neutrophilia with regenerative left shift – and a mild monocytosis.
Biochemistry is unremarkable, other than a moderate increase in alkaline phosphatase.
What are the main differential diagnoses based on the clinical examination and blood results?
The profound thrombocytopenia is the most clinically useful finding and explains the clinical signs present. Differential diagnoses include:
A diagnosis of immune-mediated thrombocytopenia (IMTP) relies on excluding other potential causes. Abdominal ultrasound and thoracic radiography were performed and found to be unremarkable. An in-house ELISA for Angiostrongylus vasorum was negative. This patient had never travelled abroad, so other infectious causes were not tested for.
As an underlying trigger could not be identified, a diagnosis of IMTP was made. The patient was given a whole blood transfusion to address the collapse and acute anaemia, and the following medication was started:
Consent was obtained from the owner before starting unlicensed medications.
This patient had an excellent response to treatment. A clinical examination and haematology were performed every two to four weeks for nine months. During this time, the platelet count remained normal. The patient tolerated the treatment very well and developed minimal side effects.
Prednisolone and azathioprine were gradually reduced and withdrawn. The patient has been stable and off medication for six months.