21 Sept 2015
Julia Henken
Job Title
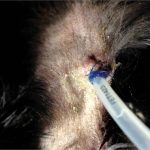
Figure 2. Oesophagostomy tube infection site.
You have just heroically placed an oesophagostomy feeding tube into a seven-year-old anorexic cat called Fifi, which has suspected triaditis.
Fifi is recovering from the anaesthetic and the nurse has asked you for a feeding and management plan for this nutritionally stubborn feline.
RER for animals 2kg to 30kg = 30 × weight in kg + 70
For dogs more than 30kg, use 70 × weight in kg0.75
For cats you can just use 40 × weight in kg
So Fifi, a 3.5kg cat, would require 140kcal/day
What management advice should you give regarding feeding tube care and nutrition?
A number of factors should be considered and you need to know a few of these to prevent some of the common pitfalls of feeding tube management.
If the animal has been anorexic for more than three days, it is prudent to prevent refeeding syndrome and gently introduce the body to the concept of food again. Do this by providing 33 per cent of resting energy requirements (RER) on day one, 66 per cent on day two and then 100 per cent on day three. For patients that have eaten more recently, you can give 50 per cent on day one and 100 per cent on day two (Panel 1).
Kcal per day / 4.73 = grams of Convalescence Support a day
So for Fifi, 140 / 4.73 = 29.6
You add three times the amount in water to make up the feed, so 29.6 × 3 = 88ml of feed per day
This amount should be divided into four to six feeds per day.
Diet-wise, a good all-rounder is Royal Canin Convalescence Support S/O. Add 150ml water to a 50g sachet to make up the feed to the correct consistency to fit down a 14F tube – 100g of the food contains 473kcal. To calculate the amount to feed per day, see Panel 2.
Convalescence contains very high protein levels, so would not be appropriate in cases of hepatic encephalopathy. In these cases, use an alternative diet (Table 1).
Ensure the feed has been warmed to body temperature before feeding. The feed must be given slowly over 10 minutes to 15 minutes and if any signs of nausea or retching ensue, it must be stopped and tried again later, as it is very easy for tubes to be vomited out.
Oesophagostomy tube dressings should be changed and the stoma site cleaned daily at the minimum as infection can occur (Figures 1 and 2). With antibiotic cover and stoma site care this can be minimised and it is not usually necessary to remove the tube.
Oesophagostomy tubes can be left in place for weeks to months and do not need to remain in place for a period of time before removal, so are often the most commonly placed. However, there are contraindications. Any disorders of the oesophagus – such as oesophagitis, oesophageal rupture and megaoesophagus – are major contraindications and in these cases it may be better to use a different technique such as a gastrostomy tube.
Any coagulation disorders such as thrombocytopaenia would need to be stabilised before any surgical interventions. In these cases, placement of a naso-oesophageal feeding tube is an easy short-term option.
So, to achieve a good outcome with a feeding tube it is important to make a sound plan.
Make a feeding chart for the staff caring for the patient detailing frequency and amount of feeds and how to prepare the feed itself. Training staff on the correct feeding technique is important as it is very common for feed to be given too quickly, which can lead to regurgitation and aspiration.


Good feeding tube management will lead to quicker patient recovery, and reduced morbidity and hospitalisation times. Fifi was discharged with the tube in place and the clients gave her feeds at home until she began eating well on her own and fully recovered.