2 Dec 2019
Sarah Caney discusses this common presentation in cats – including information to advise owners and treatment innovations.
Sarah Caney
Job Title
Figure 1. Peripheral neuropathy – typically manifested as a plantigrade stance – is a potential long-term complication of diabetes mellitus.
Diabetes is the second most common feline endocrinopathy – after hyperthyroidism – and estimated to affect approximately 1 in 200 UK cats. It is believed its prevalence is increasing.
Diabetes is a complicated condition caused by either an absolute or relative deficiency of insulin, which results in hyperglycaemia and glycosuria. Typical clinical signs associated with diabetes include polydipsia, polyuria, polyphagia and weight loss.
Management – primarily through use of insulin and a therapeutic “diabetic” diet – aims for diabetic remission, if possible. Recent data reported a median survival time of 516 days, with almost half of the diabetic cats living for more than two years.
The majority of diabetic cats are non-ketotic and their diabetes is analogous to human type-two diabetes mellitus – characterised by insulin resistance, obesity and pancreatic amyloid deposition.
Ketoacidotic diabetic cats need to be treated urgently, with attention to electrolyte imbalances (potassium, phosphate), fluid therapy, and reversing the hyperglycaemia and ketoacidosis.
Diagnosis of diabetes mellitus is often suspected on the basis of the clinical history.
A UK study has reported an increased risk of diabetes in certain breeds, including the Tonkinese, Burmese and Norwegian forest (O’Neill et al, 2016).
Physical examination may be unremarkable, or changes may be present – including hepatomegaly, abdominal distension and evidence of peripheral neuropathy (Figure 1).
Confirmation of the diagnosis requires blood and urinalysis to confirm hyperglycaemia and glycosuria; however, this can be complicated by the stress hyperglycaemia phenomenon.
Struggling and vocalising during handling increases the likelihood of a stress-associated increase in blood glucose. Although usually relatively mild in nature, in some cats the stress increase in glucose can result in severe hyperglycaemia and glycosuria.
If glucose and ketones are present in the urine of a hyperglycaemic cat, this confirms diabetes mellitus. Otherwise, confirmation of the diabetes may require further steps – such as collection of a urine sample by the owner at home a few days later. If negative for glucose, this would be consistent with a previous stress-associated hyperglycaemia.
Alternatively, consideration can be given to analysing levels of glycosylated serum proteins (fructosamine) or glycated haemoglobin (A1C), both of which give a longer-term indication of blood glucose levels.
Fructosamine is a glycosylated serum protein molecule produced by a non-enzymatic reaction between glucose and the amino groups of plasma proteins. The concentration of fructosamine depends on plasma glucose concentrations for the preceding one to two weeks and the circulating half-lives of plasma proteins – for example, albumin has a half-life of about three weeks.
Fructosamine levels are elevated when the blood glucose concentration is high for a prolonged period – and an elevation in serum fructosamine indicates significant hyperglycaemia during the previous one to three weeks.

Fructosamine estimation is, therefore, very helpful for differentiating stress hyperglycaemia from hyperglycaemia associated with diabetes when diagnosing new cases and monitoring long-term control in existing patients.
Levels of fructosamine can be affected by a number of factors – an artefactual reduction in fructosamine levels occurs in hyperthyroid cats due to accelerated protein turnover, so this test needs to be interpreted with care in these cats.
Hypoproteinaemia will also depress fructosamine levels, but, in contrast to dogs, serum fructosamine levels are not affected by hyperlipidaemia, hypertriglyceridaemia or azotaemia.
Once a diagnosis of diabetes mellitus has been confirmed, treatment can begin. The goals of diabetic stabilisation are:
If possible, achievement of diabetic remission.
Resolution of clinical signs associated with diabetes mellitus – polyuria, polydipsia, polyphagia and weight loss being the major ones.
Maintaining blood glucose levels below the renal threshold (12mmol/L to 14mmol/L) for the majority of the time. This should be associated with prevention/minimisation of ketoacidosis and the development of other long-term complications of diabetes, such as peripheral neuropathies.
Avoid hypoglycaemia by maintaining blood glucose levels above 5mmol/L.
Early diagnosis and aggressive treatment increase the chances of diabetic remission. Efforts should, therefore, be concentrated on:
Insulin therapy and dietary management. Resolution of glucose toxicity greatly increases the chance of achieving diabetic remission. Glucose toxicity describes the situation whereby prolonged hyperglycaemia suppresses insulin secretion by the β-cells of the pancreas. As glucose toxicity resolves, the β-cells may recover some ability to produce and secrete insulin, leading to improved glycaemic control and diabetic remission in some patients.
Where possible, withdrawing diabetogenic drugs the cat may be receiving – for example, glucocorticoids.
Managing obesity, where present. Obesity causes insulin resistance and is an important risk factor for the development of feline diabetes.
Identifying and supporting concurrent diseases, where present. Therefore – additionally to a history and physical examination – haematology, serum biochemistry, total thyroxine and urinalysis (including bacterial culture) are recommended where possible. Urinary tract infections (UTIs) are a potential complication of diabetes, and will increase insulin requirements and complicate stabilisation. The reported prevalence of bacterial UTIs in cats with diabetes mellitus has varied from 7% to 14.3% (Bailiff et al, 2006; Michiels et al, 2008; Mayer-Roenne et al, 2007; Bailiff et al, 2008).
Typically, a third to half of diabetic cats treated with insulin may achieve diabetic remission and are able to maintain normoglycaemia without insulin therapy or use of other glucose-lowering drugs (Michiels et al, 2008; Gostelow et al, 2014; Hazuchova et al, 2018).
Evidence exists that early intensive management with long-acting insulin (glargine or detemir) and dietary management can increase this figure to greater than 80% in some situations (Roomp and Rand, 2009; Marshall et al, 2009; Roomp and Rand, 2012; Gostelow et al, 2014).
Diabetic remission is also possible for patients presenting in diabetic ketoacidosis. Remission typically occurs within one month to three months of initiation of treatment, although relapse occurs transiently or permanently in about a quarter of these. Remission from relapse is generally much more difficult to achieve.
Studies have shown benefits to glycaemic control by feeding diabetic cats a low-carbohydrate diet. These studies reported diabetic remission rates between 33% and 100% when using a combination of dietary management and insulin therapy (Roomp and Rand, 2009; 2012; Marshall et al, 2009).
A number of specially formulated veterinary prescription diets are available for this purpose. Wet diets are generally recommended over dry because these often contain lower carbohydrate levels. The lower energy density and greater water content is also useful for managing obesity.
Use of low-carbohydrate diets may reduce or eliminate the need for insulin therapy in the long term. In those cats where the diet is changed following diagnosis of diabetes, it is important to do this slowly and monitor the patient carefully, since insulin requirements can change very quickly.
Low-carbohydrate diets are suitable for use in diabetic cats of all weights – whether needing weight loss or gain. Since cats have a very prolonged postprandial glycaemia, timing of meals is not critical for the management of most feline diabetic patients.
Insulin therapy is required to stabilise most diabetic cats.
In general, twice-daily insulin therapy is associated with better results than once-daily, regardless of the insulin preparation chosen – although considerable inter-cat variation exists in duration of action and response to insulin.
Longer-acting insulins are generally recommended for the treatment of diabetic cats, where possible (Sparkes et al, 2015; Behrend et al, 2018).
The two veterinary licensed insulins in the UK are:
Longer-acting protamine zinc insulin: a recombinant human insulin in a 40IU/ml formulation and typical duration of between 13 hours and 24 hours. Some studies have indicated improved glycaemic control when using twice-daily protamine zinc insulin compared to twice-daily lente insulin (Gostelow et al, 2018) and this should be prioritised for cats with a short duration of action on lente.
Medium-acting lente insulin: this is a porcine insulin zinc suspension, with an insulin concentration of 40IU/ml and typical duration of between 8 hours and 10 hours. It provides good to excellent clinical control of diabetes in the majority of patients.
When using 40IU/ml preparations, it is essential to also use 40IU/ml syringes. Use of a magnifying glass or reading spectacles can be helpful for care providers with poor eyesight, especially when low doses are prescribed.
Medium-acting lente insulin is available in a pen doser that accurately dispenses insulin in 0.5IU increments. Pens facilitate more accurate dosing, especially when a low dose is required, helping to reduce the risk of hypoglycaemia (Thompson et al, 2015).
Use of pens is associated with fewer needlestick injuries, although carers do not always find them easier to use (Albuquerque et al, 2019).
Most cats require only small doses of insulin. Non-ketotic diabetic cats should be started on insulin at a dose of around 0.25 units to 0.5 units per kilogram bodyweight per injection (maximum starting dose 2IU per cat).
The dose of insulin should not be increased more often than every five days as it takes several days for the effects of a new dose to “settle out”.
Detailed guidelines for diabetic stabilisation and monitoring are available elsewhere (Sparkes et al, 2015; Behrend et al, 2018).
Owners can play a vital role in monitoring the success of therapy in their diabetic cat.
Home monitoring of glucose has been shown to have a positive impact on management. This can include blood glucose checks using a marginal ear vein.
More recently, continuous glucose monitoring devices have become available on the human market, and are being used in diabetic cats and dogs (Corradini et al, 2016). These systems involve placing a sensor – typically over the back of the cat’s neck, which can stay in place for up to two weeks – continuously measuring interstitial fluid glucose levels that can be read using a smartphone app.
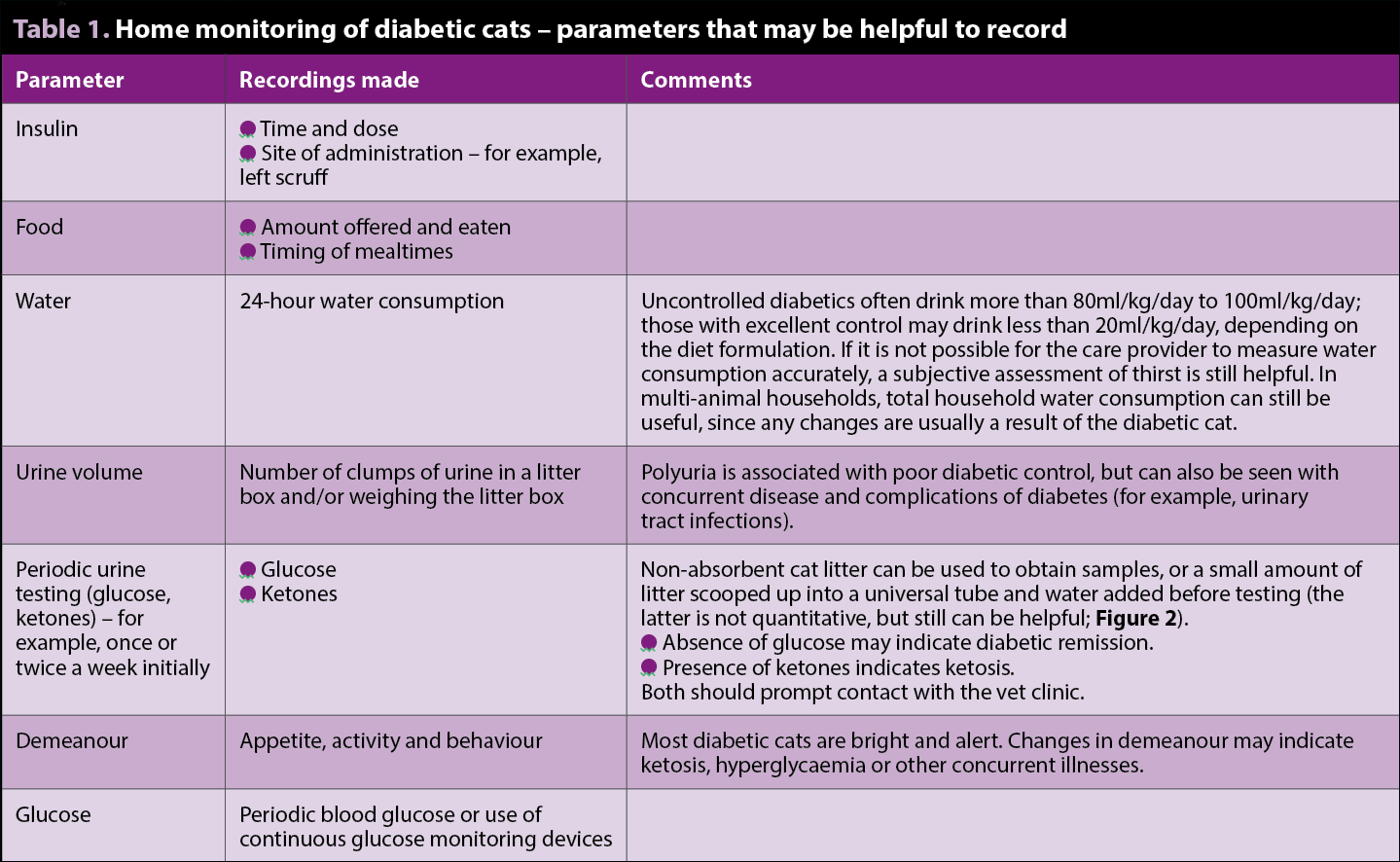
Periodic home monitoring of urine is less helpful – other than confirming diabetic remission (absence of glucose) and ketosis, both of which should prompt immediate contact with the veterinary clinic for further advice.
Monitoring water intake often provides useful information on diabetic stabilisation, with good control being associated with a normal water intake. It is helpful if owners keep a diary recording all of this information, as well as timing and the dose of insulin administered (Table 1).
Owner education should include information regarding recognition and management of hypoglycaemia and ketosis.
Signs of hypoglycaemia include weakness, ataxia, tremors and seizures. Care providers should be instructed in signs to look for and action to take, which includes not injecting any more insulin, providing the cat with food and – if the cat does not eat – applying glucose or sugar solution to the gums. It is sensible to provide carers with glucose powder or solution to keep at home in the event of hypoglycaemia.
Many cases of diabetes are straightforward to stabilise, although it may take several weeks or months to identify an optimal insulin regime.
Dietary management – ideally involving feeding a therapeutic diet – improves patient outcome.
Early diagnosis and treatment increases the chances of diabetic remission.
Detailed survival statistics for diabetic cats are not available, but one study has reported a median survival time of 516 days; almost half of the cats lived for more than two years (Callegari et al, 2013).
Some drugs in this article are used under the cascade.